

Risk factors for revision within 10 years of total knee arthroplasty
- PMID: 24347046
- PMCID: PMC3940740
- DOI: 10.1007/s11999-013-3416-6
Risk factors for revision within 10 years of total knee arthroplasty
Abstract
Background: An in-depth understanding of risk factors for revision TKA is needed to minimize the burden of revision surgery. Previous studies indicate that hospital and community characteristics may influence outcomes after TKA, but a detailed investigation in a diverse population is warranted to identify opportunities for quality improvement.
Questions/purposes: We asked: (1) What is the frequency of revision TKA within 10 years of primary arthroplasty? (2) Which patient demographic factors are associated with revision within 10 years of TKA? (3) Which community and institutional characteristics are associated with revision within 10 years of TKA?
Methods: We identified 301,955 patients who underwent primary TKAs in New York or California from 1997 to 2005 from statewide databases. Identifier codes were used to determine whether they underwent revision TKA. Patient, community, and hospital characteristics were analyzed using multivariable regression modeling to determine predictors for revision.
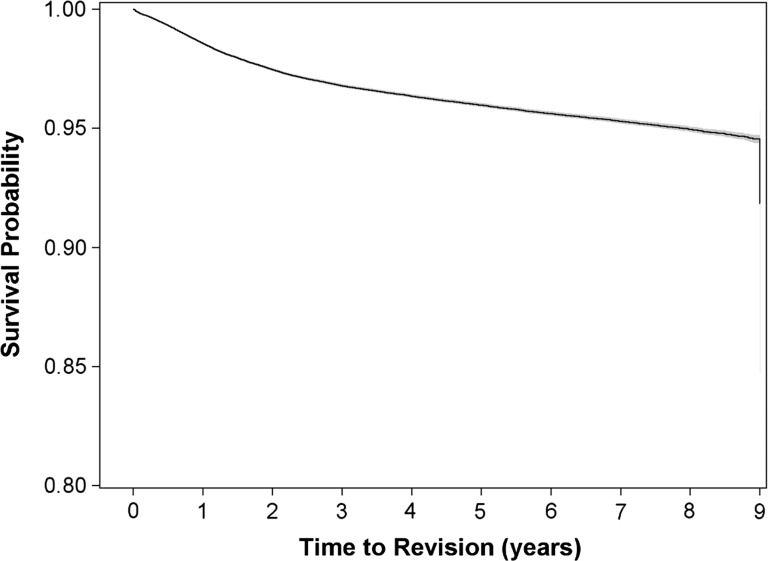
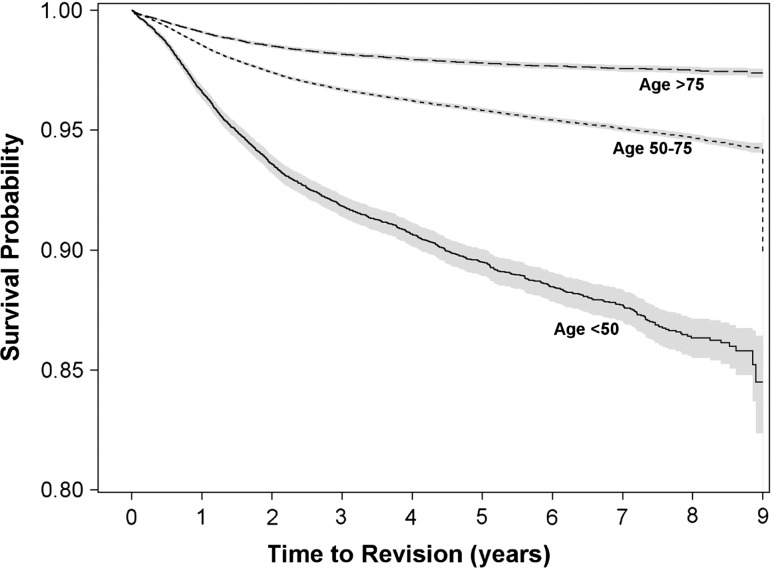
Results: The frequency of revision was 4.0% at 5 years after the index arthroplasty and 8.9% at 9-years. Patients between 50 and 75 years old had a lower risk of revision than patients younger than 50 years (hazard ratio [HR], 0.47; 95% CI, 0.44, 0.50). Black patients were at increased risk for needing revision surgery (HR, 1.39; 95% CI, 1.29, 1.49) after adjustment for insurance type, poverty level, and education. Women (HR, 0.82; 95% CI, 0.79, 0.86) and Medicare recipients (HR, 0.82; 95% CI, 0.79, 0.86) were less likely to undergo revision surgery, whereas those from the most educated (HR, 1.09; 95% CI, 1.02, 1.16) and the poorest communities (HR, 1.08; 95% CI, 1.01, 1.15) had modest increases in risk of revision. Mid-volume hospitals (200-400 annual cases) had a reduction of early revision (HR, 0.91; 95% CI, 0.83, 0.99) compared with those performing less than 200 cases annually, whereas higher-volume hospitals (greater than 400 cases) showed little effect compared with low-volume hospitals.
Conclusions: Patient, community, and institutional characteristics affect the risk for revision within 10 years of index TKA. These data can be used to develop process improvement and implant surveillance strategies among high-risk patients.
Level of evidence: Level III, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Figures
Comment in
-
CORR Insights(®): Risk factors for revision within 10 years of total knee arthroplasty.Clin Orthop Relat Res. 2014 Apr;472(4):1208-9. doi: 10.1007/s11999-013-3450-4. Epub 2014 Feb 14. Clin Orthop Relat Res. 2014. PMID: 24526297 Free PMC article. No abstract available.
References
-
- Bang H, Chiu YL, Memtsoudis SG, Mandl LA, Della Valle AG, Mushlin AI, Marx RG, Mazumdar M. Total hip and total knee arthroplasties: trends and disparities revisited. Am J Orthop (Belle Mead NJ). 2010;39:E95–E102. - PubMed
-
- Bozic KJ, Kinder J, Meneghini RM, Zurakowski D, Rosenberg AG, Galante JO. Implant survivorship and complication rates after total knee arthroplasty with a third-generation cemented system: 5 to 8 years followup. Clin Orthop Relat Res. 2005;430:117–124. doi: 10.1097/01.blo.0000146539.23869.14. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
