

Transoesophageal Doppler compared to central venous pressure for perioperative hemodynamic monitoring and fluid guidance in liver resection
- PMID: 24348287
- PMCID: PMC3858686
- DOI: 10.4103/1658-354X.121044
Transoesophageal Doppler compared to central venous pressure for perioperative hemodynamic monitoring and fluid guidance in liver resection
Erratum in
- Saudi J Anaesth. 2014;8(1):133
Abstract
Purpose: Major hepatic resections may result in hemodynamic changes. Aim is to study transesophageal Doppler (TED) monitoring and fluid management in comparison to central venous pressure (CVP) monitoring. A follow-up comparative hospital based study.
Methods: 59 consecutive cirrhotic patients (CHILD A) undergoing major hepatotomy. CVP monitoring only (CVP group), (n=30) and TED (Doppler group), (n=29) with CVP transduced but not available on the monitor. Exclusion criteria include contra-indication for Doppler probe insertion or bleeding tendency. An attempt to reduce CVP during the resection in both groups with colloid restriction, but crystalloids infusion of 6 ml/kg/h was allowed to replace insensible loss. Post-resection colloids infusion were CVP guided in CVP group (5-10 mmHg) and corrected flow time (FTc) aortic guided in Doppler group (>0.4 s) blood products given according to the laboratory data.
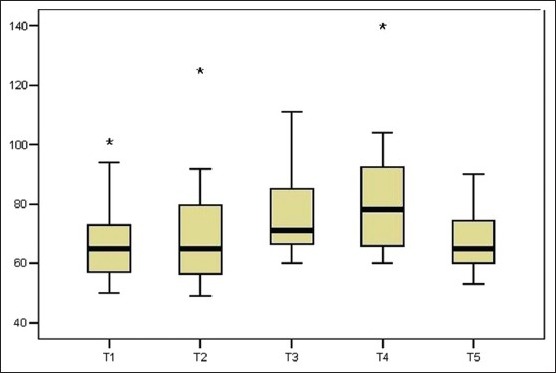
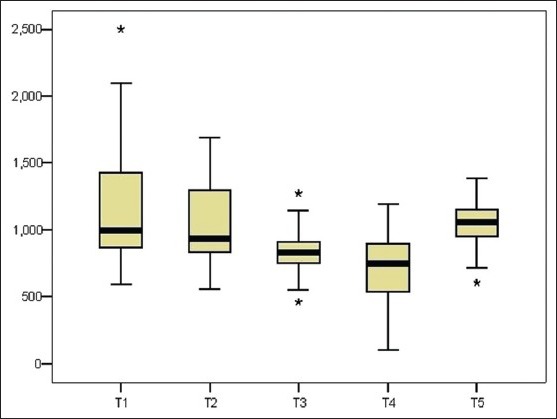
Results: Using the FTc to guide Hydroxyethyl starch 130/0.4 significantly decreased intake in TED versus CVP (1.03 [0.49] versus 1.74 [0.41] Liter; P<0.05). Nausea, vomiting, and chest infection were less in TED with a shorter hospital stay (P<0.05). No correlation between FTc and CVP (r=0.24, P > 0.05). Cardiac index and stroke volume of TED increased post-resection compared to baseline, 3.0 (0.9) versus 3.6 (0.9) L/min/m(2), P<0.05; 67.1 (14.5) versus 76 (13.2) ml, P<0.05, respectively, associated with a decrease in systemic vascular resistance (SVR) 1142.7 (511) versus 835.4 (190.9) dynes.s/cm(5), P<0.05. No significant difference in arterial pressure and CVP between groups at any stage. CVP during resection in TED 6.4 (3.06) mmHg versus 6.1 (1.4) in CVP group, P=0.6. TED placement consumed less time than CVP (7.3 [1.5] min versus 13.2 [2.9], P<0.05).
Conclusion: TED in comparison to the CVP monitoring was able to reduced colloids administration post-resection, lower morbidity and shorten hospital stay. TED consumed less time to insert and was also able to present significant hemodynamic changes. Advanced surgical techniques of resection play a key role in reducing blood loss despite CVP more than 5 cm H2O. TED fluid management protocols during resection need to be developed.
Keywords: Central venous pressure; liver resection; monitoring; transoesophageal Doppler.
Conflict of interest statement
Figures
Similar articles
-
Effect of intraoperative transesophageal Doppler-guided fluid therapy versus central venous pressure-guided fluid therapy on renal allograft outcome in patients undergoing living donor renal transplant surgery: a comparative study.J Anesth. 2015 Dec;29(6):842-9. doi: 10.1007/s00540-015-2046-4. Epub 2015 Jul 28. J Anesth. 2015. PMID: 26216743
-
THE BENEFICIAL VALUES OF TRANSOESOPHAGEAL DOPPLER IN INTRAOPERATIVE FLUID GUIDANCE VERSUS STANDARD CLINICAL MONITORING PARAMETERS IN INFANTS UNDERGOING KASAI OPERATION.Middle East J Anaesthesiol. 2015 Oct;23(3):331-7. Middle East J Anaesthesiol. 2015. PMID: 26860024 Clinical Trial.
-
THE BENEFICIAL VALUES OF TRANSOESOPHAGEAL DOPPLER IN INTRAOPERATIVE FLUID GUIDANCE VERSUS STANDARD CLINICAL MONITORING PARAMETERS IN INFANTS UNDERGOING KASAI OPERATION.Middle East J Anaesthesiol. 2015 Jun;23(2):205-11. Middle East J Anaesthesiol. 2015. PMID: 26442398 Clinical Trial.
-
Perioperative hemodynamic monitoring with transesophageal Doppler technology.Anesth Analg. 2009 Aug;109(2):340-53. doi: 10.1213/ane.0b013e3181aa0af3. Anesth Analg. 2009. PMID: 19608800 Review.
-
Low versus standard central venous pressure during laparoscopic liver resection: A systematic review, meta-analysis and trial sequential analysis.Ann Hepatobiliary Pancreat Surg. 2024 May 31;28(2):115-124. doi: 10.14701/ahbps.23-137. Epub 2024 Feb 16. Ann Hepatobiliary Pancreat Surg. 2024. PMID: 38361339 Free PMC article. Review.
Cited by
-
Restricted Versus Liberal Versus Goal-Directed Fluid Therapy for Non-vascular Abdominal Surgery: A Network Meta-Analysis and Systematic Review.Cureus. 2023 Apr 28;15(4):e38238. doi: 10.7759/cureus.38238. eCollection 2023 Apr. Cureus. 2023. PMID: 37261162 Free PMC article. Review.
-
Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials.Crit Care. 2017 Jun 12;21(1):141. doi: 10.1186/s13054-017-1728-8. Crit Care. 2017. PMID: 28602158 Free PMC article.
-
Goal-directed haemodynamic therapy (GDHT) in surgical patients: systematic review and meta-analysis of the impact of GDHT on post-operative pulmonary complications.Perioper Med (Lond). 2020 Oct 15;9:30. doi: 10.1186/s13741-020-00161-5. eCollection 2020. Perioper Med (Lond). 2020. PMID: 33072306 Free PMC article.
-
Goal-directed haemodynamic therapy during general anaesthesia for noncardiac surgery: a systematic review and meta-analysis.Br J Anaesth. 2022 Mar;128(3):416-433. doi: 10.1016/j.bja.2021.10.046. Epub 2021 Dec 13. Br J Anaesth. 2022. PMID: 34916049 Free PMC article.
-
Effect of intraoperative magnesium intravenous infusion on the hemodynamic changes associated with right lobe living donor hepatotomy under transesophageal Doppler monitoring-randomized controlled trial.Saudi J Anaesth. 2016 Apr-Jun;10(2):132-7. doi: 10.4103/1658-354X.168799. Saudi J Anaesth. 2016. PMID: 27051361 Free PMC article.
References
-
- Buell JF, Rosen S, Yoshida A, Labow D, Limsrichamrern S, Cronin DC, et al. Hepatic resection: Effective treatment for primary and secondary tumors. Surgery. 2000;128:686–93. - PubMed
-
- Chiappa A, Zbar AP, Audisio RA, Leone BE, Biella F, Staudacher C. Factors affecting survival and long-term outcome in the cirrhotic patient undergoing hepatic resection for hepatocellular carcinoma. Eur J Surg Oncol. 2000;26:387–92. - PubMed
-
- Weber SM, Jarnagin WR, DeMatteo RP, Blumgart LH, Fong Y. Survival after resection of multiple hepatic colorectal metastases. Ann Surg Oncol. 2000;7:643–50. - PubMed
-
- Brancatisano R, Isla A, Habib N. Is radical hepatic surgery safe? Am J Surg. 1998;175:161–3. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
