

Transabdominal ultrasonography of the small bowel
- PMID: 24348544
- PMCID: PMC3852808
- DOI: 10.1155/2013/896704
Transabdominal ultrasonography of the small bowel
Abstract
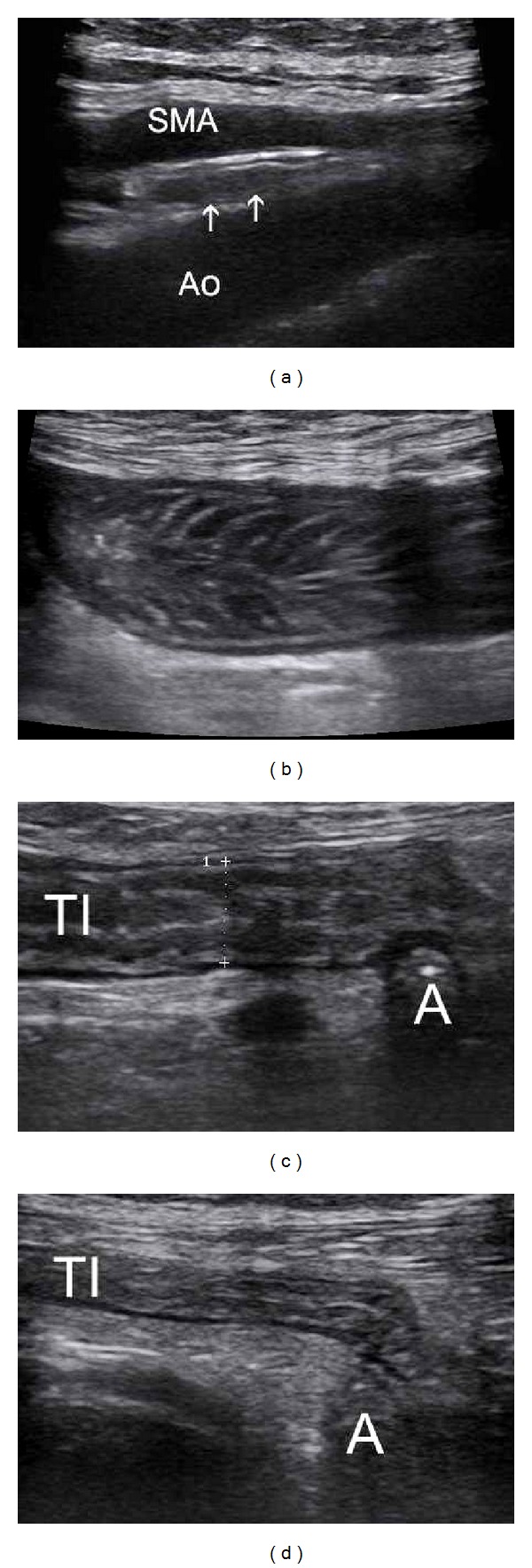
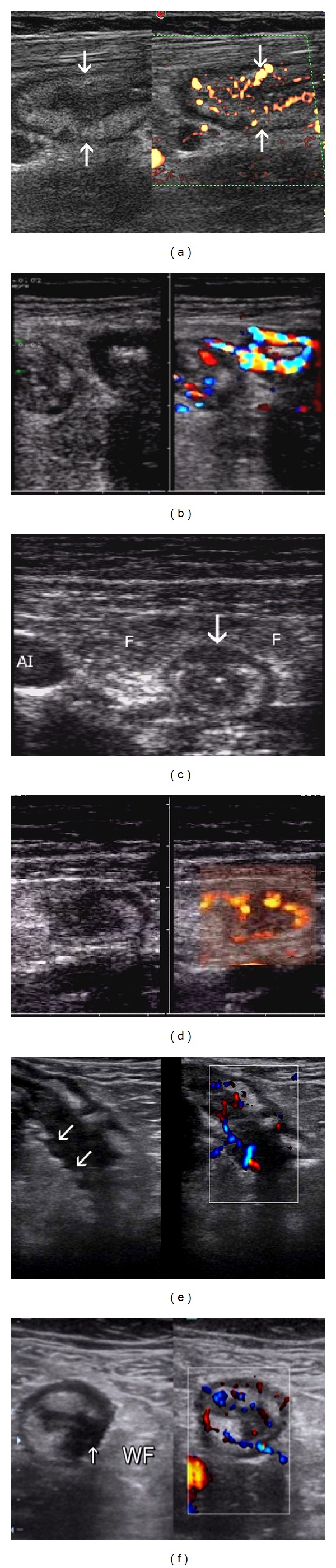
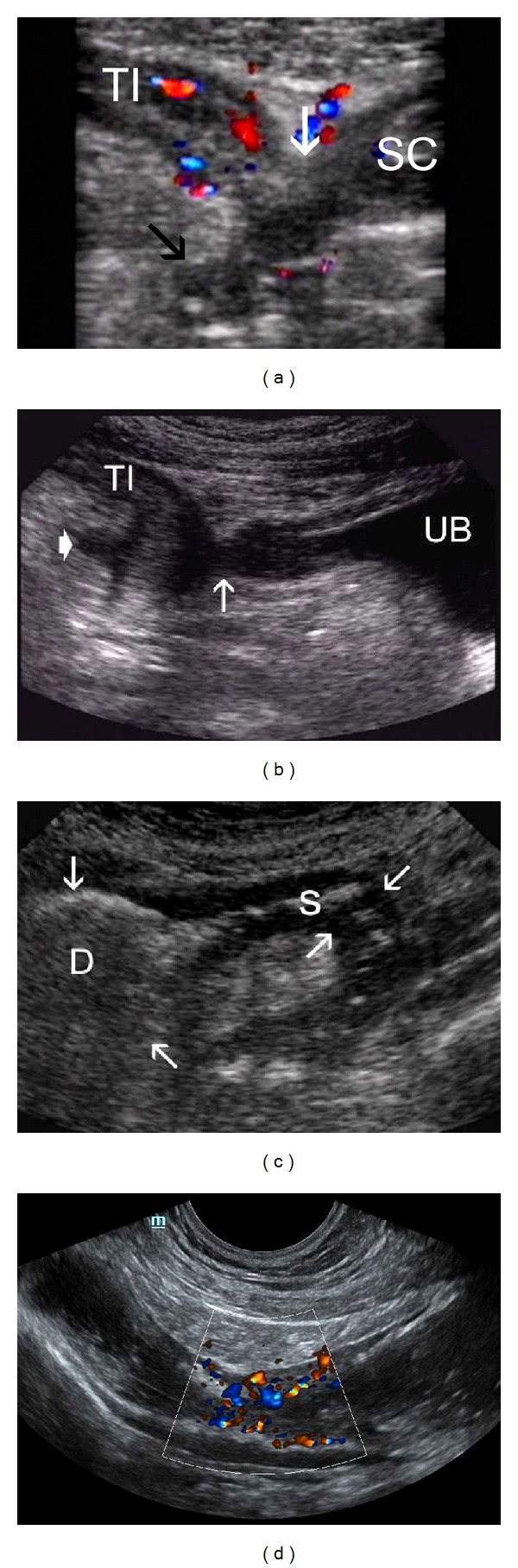
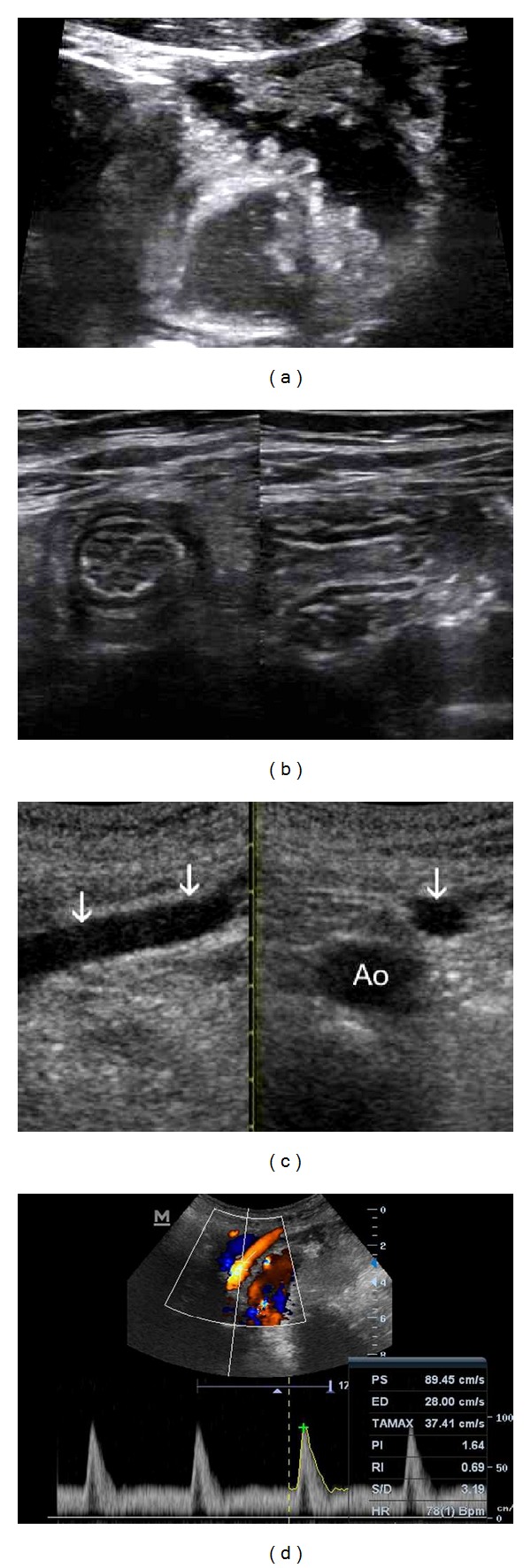
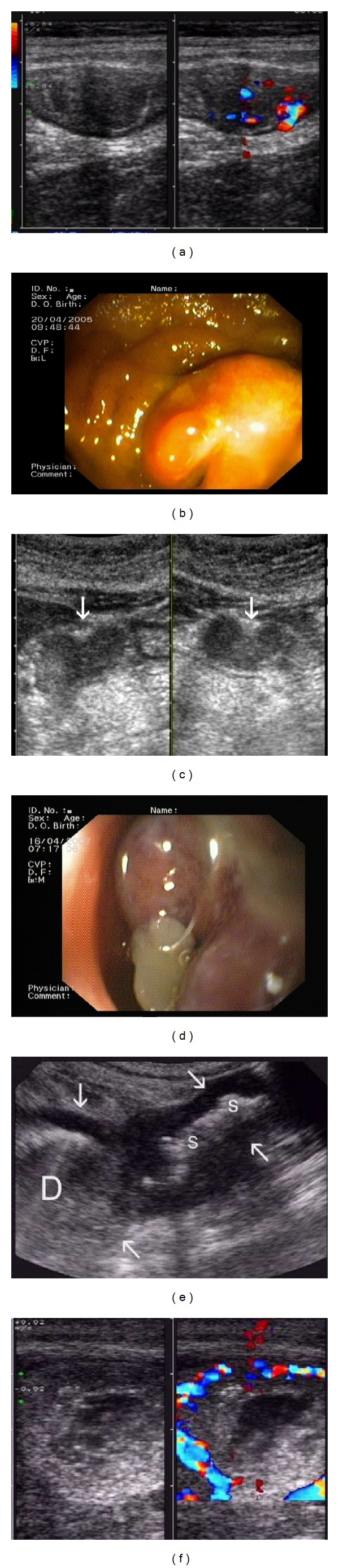
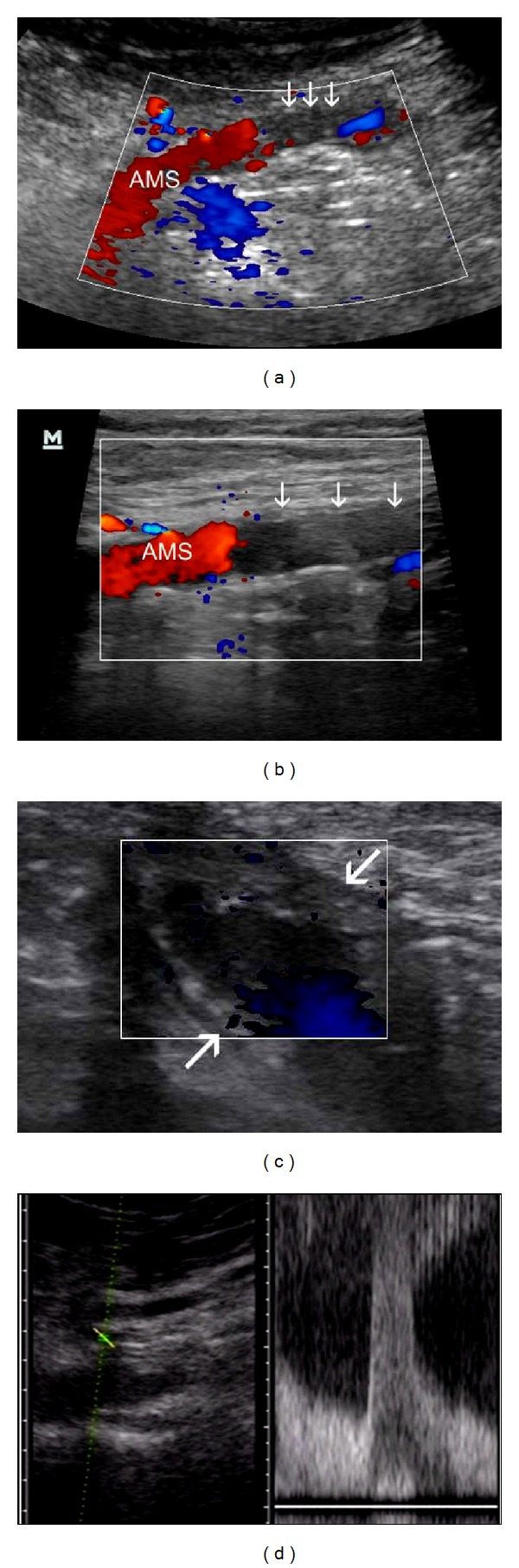
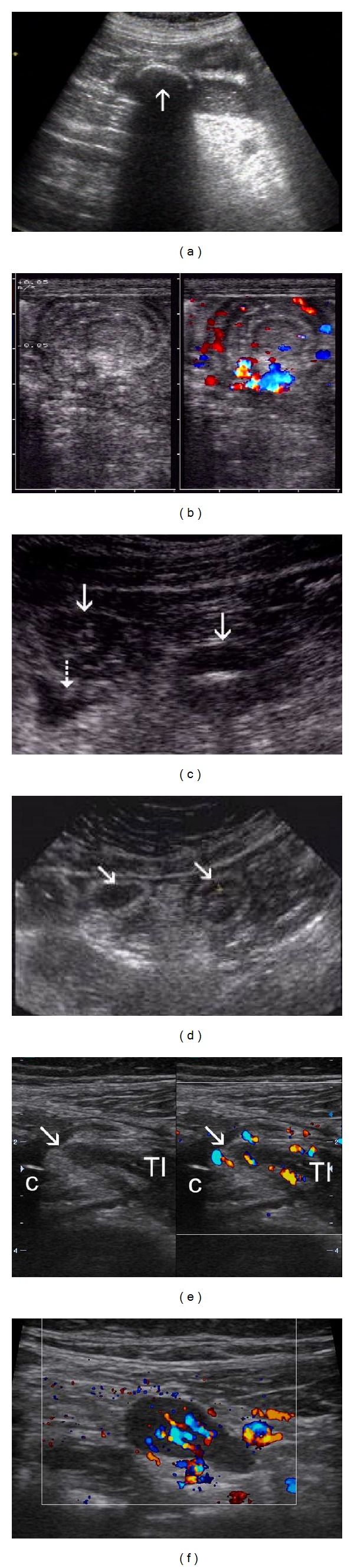
In the era of double balloon enteroscopy, capsule endoscopy, CT, and MRI enterography is transabdominal ultrasonography (TUS) underestimated method for evaluation of small bowel pathology. As often initial imagine method in abdominal complaints, nowadays has TUS much better diagnostic potential than two decades ago. High-resolution ultrasound probes with harmonic imaging significantly improve resolution of bowel wall in real time, with possibility to asses bowel peristalsis. Color flow doppler enables evaluation of intramural bowel vascularisation, pulse wave doppler helps to quantificate flow in coeliac and superior mesenteric arteries. Small intestine contrast ultrasonography with oral contrast fluid, as well as contrast enhanced ultrasonography with intravenous microbubble contrast also improves small bowel imaging. We present a review of small intestine pathology that should be detected during ultrasound examinations, discuss technical requirements, advantages and limitations of TUS, typical ultrasound signs of Crohn's disease, ileus, celiac disease, intussusception, infectious enteritis, tumours, ischemic and haemorrhagic conditions of small bowel. In the hands of experienced investigator, despite some significant limitations(obesity, meteorism), is transabdominal ultrasonography reliable, noninvasive and inexpensive alternative method to computerised tomography (CT) and magnetic resonance imaging (MRI) in small bowel examination.
Figures
Similar articles
-
Clinical usefulness of transabdominal ultrasonography prior to patency capsule for suspected small-bowel strictures.Scand J Gastroenterol. 2016 Mar;51(3):281-7. doi: 10.3109/00365521.2015.1095942. Epub 2015 Oct 14. Scand J Gastroenterol. 2016. PMID: 26466551
-
Ultrasound of selected pathologies of the small intestine.J Ultrason. 2013 Jun;13(53):155-66. doi: 10.15557/JoU.2013.0016. Epub 2013 Jun 30. J Ultrason. 2013. PMID: 26672622 Free PMC article.
-
Clinical usefulness of classification by transabdominal ultrasonography for detection of small-bowel stricture.Scand J Gastroenterol. 2013 Sep;48(9):1041-7. doi: 10.3109/00365521.2013.822546. Epub 2013 Aug 2. Scand J Gastroenterol. 2013. PMID: 23906185
-
Small bowel imaging - still a radiologic approach?Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010 Jun;154(2):123-32. doi: 10.5507/bp.2010.019. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010. PMID: 20668493 Review.
-
Small bowel imaging in celiac disease.Gastrointest Endosc Clin N Am. 2012 Oct;22(4):735-46. doi: 10.1016/j.giec.2012.07.013. Epub 2012 Aug 28. Gastrointest Endosc Clin N Am. 2012. PMID: 23083990 Review.
Cited by
-
Beneficial effects of combining computed tomography enteroclysis/enterography with capsule endoscopy for screening tumor lesions in the small intestine.Gastroenterol Res Pract. 2015;2015:952787. doi: 10.1155/2015/952787. Epub 2015 Feb 22. Gastroenterol Res Pract. 2015. PMID: 25792979 Free PMC article.
-
The role of intestinal ultrasound in diagnostics of bowel diseases.Prz Gastroenterol. 2018;13(1):1-5. doi: 10.5114/pg.2018.74554. Epub 2018 Mar 26. Prz Gastroenterol. 2018. PMID: 29657604 Free PMC article. Review.
-
Role of ultrasound in colorectal diseases.World J Gastroenterol. 2016 Nov 21;22(43):9477-9487. doi: 10.3748/wjg.v22.i43.9477. World J Gastroenterol. 2016. PMID: 27920469 Free PMC article. Review.
-
Predictive value of transabdominal intestinal sonography in critically ill patients: a prospective observational study.Crit Care. 2019 Nov 27;23(1):378. doi: 10.1186/s13054-019-2645-9. Crit Care. 2019. PMID: 31775838 Free PMC article.
-
Intestinal stricture in Crohn's disease.Intest Res. 2015 Jan;13(1):19-26. doi: 10.5217/ir.2015.13.1.19. Epub 2015 Jan 29. Intest Res. 2015. PMID: 25691840 Free PMC article. Review.
References
-
- Schmidt T, Hohl C, Haage P, et al. Phase-inversion tissue harmonic imaging compared to fundamental B-mode ultrasound in the evaluation of the pathology of large and small bowel. European Radiology. 2005;15(9):2021–2030. - PubMed
-
- Kuzmich S, Howlett DC, Andi A, Shah D, Kuzmich T. Transabdominal sonography in assessment of the bowel in adults. American Journal of Roentgenology. 2009;192(1):197–212. - PubMed
-
- Horsthuis K, Bipat S, Bennink RJ, Stoker J. Inflammatory bowel disease diagnosed with US, MR, scintigraphy, and CT: meta-analysis of prospective studies. Radiology. 2008;247(1):64–79. - PubMed
-
- Kimmey MB, Martin RW, Haggitt RC, Wang KY, Franklin DW, Silverstein FE. Histologic correlates of gastrointestinal ultrasound images. Gastroenterology. 1989;96(2):433–441. - PubMed
-
- Pallotta N, Baccini F, Corazziari E. Small intestine contrast ultrasonography. Journal of Ultrasound in Medicine. 2000;19(1):21–26. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
