

Endovascular stent placement of juxtaanastomotic stenosis in native arteriovenous fistula after unsuccessful balloon angioplasty
- PMID: 24348598
- PMCID: PMC3857975
- DOI: 10.5812/iranjradiol.11386
Endovascular stent placement of juxtaanastomotic stenosis in native arteriovenous fistula after unsuccessful balloon angioplasty
Abstract
Background: In hemodialysis patients, the most common problem in arteriovenous fistulas, as the best functional vascular access, is the juxtaanastomotic located lesions. Percutaneous transluminal angioplasty is accepted as the treatment method for juxtanastomotic lesions.
Objectives: To assess juxtaanastomotic stent placement after insufficient balloon angioplasty in the treatment of autogenous radiocephalic or brachiocephalic fistula dysfunction.
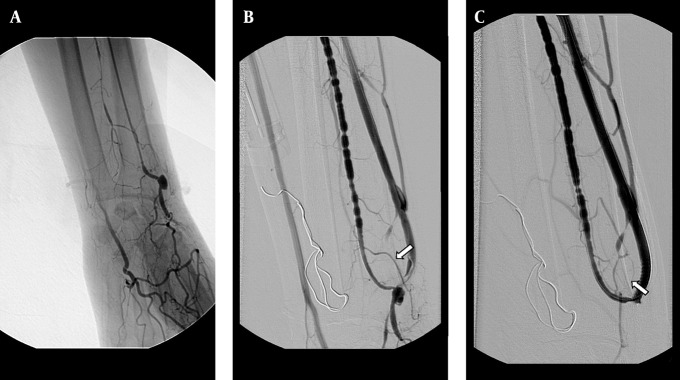
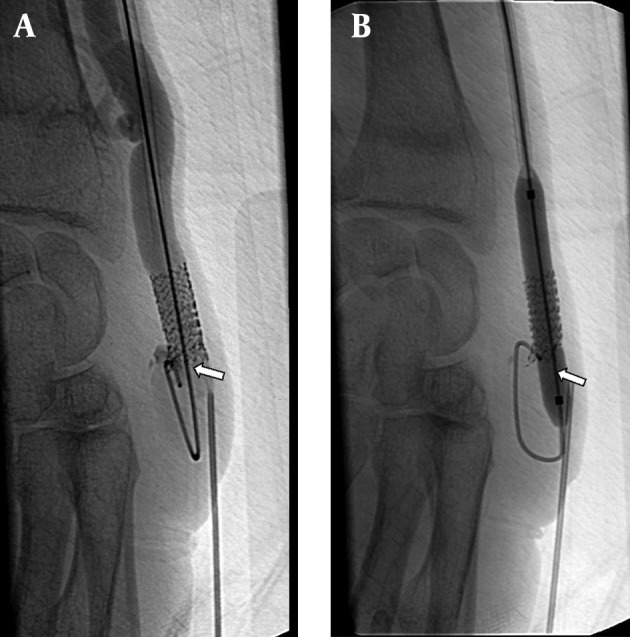
Patients and methods: Between July 2003 and June 2010, 20 hemodialysis patients with autogenous radiocephalic or brachiocephalic fistula dysfunction underwent stent placement for the lesion located at the juxtaanastomotic region. Indications for stent placement were insufficient balloon dilatation, early recurring stenosis, chronic organizing thrombus and vessel rupture. The Kaplan-Meier method was used to calculate the stent patency rates. All patients who had fistula dysfunction (thrombosis of hemodialysis access, difficult access cannulation, extremity pain due to thrombosis or decreased arterial access blood flow) were evaluated by color Doppler ultrasound. The stenoses were initially dilated with standard noncompliant balloons (3 to 10-mm in diameter). Dilatation was followed by high pressure (Blue Max, Boston Scientific) or cutting balloons (Boston Scientific), if the standard balloon failed to dilate the stenotic segment.
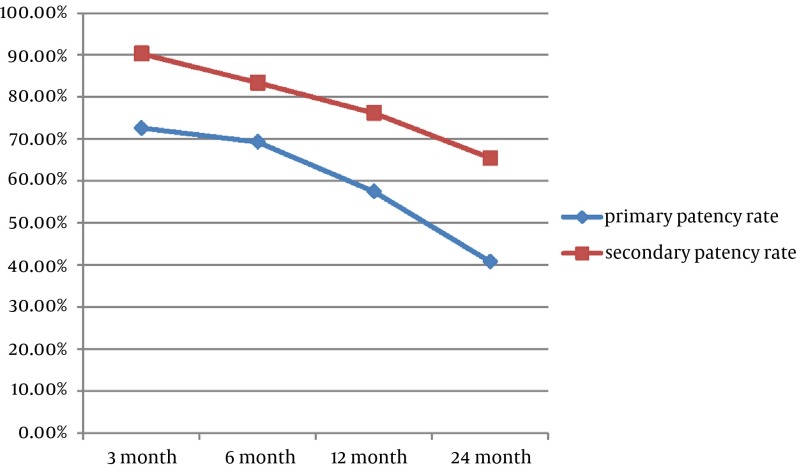
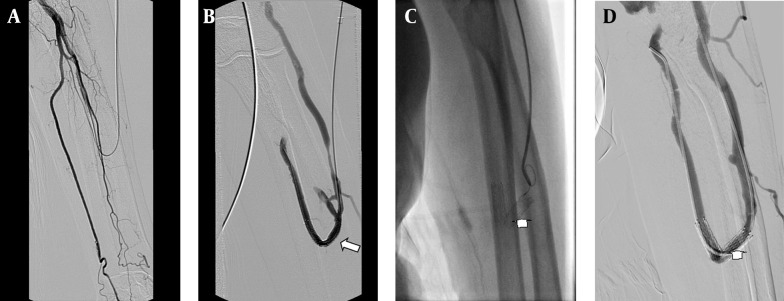
Results: Twenty-one stents were applied. The anatomical and clinical success rate was 100%. Seventeen additional interventions were done for 11 (55%) patients due to stent thrombosis or stenosis during follow-up. Our 1- and 2-year secondary patency rates were 76.2% and 65.5%, respectively and were comparable to those after balloon angioplasty and surgical shunt revision.
Conclusion: Metallic stent placement is a safe and effective procedure for salvage of native hemodialysis fistula after unsuccessful balloon angioplasty.
Keywords: Angioplasty; Endovascular Procedures; Vascular Fistula.
Figures
References
-
- Kwun KB, Schanzer H, Finkler N, Haimov M, Burrows L. Hemodynamic Evaluation of Angioaccess Procedures for Hemodialysis. Vasc Endovasc Surg. 1979;13(3):170–177. doi: 10.1177/153857447901300305. - DOI
-
- Shoenfeld R, Hermans H, Novick A, Brener B, Cordero P, Eisenbud D, et al. Stenting of proximal venous obstructions to maintain hemodialysis access. J Vasc Surg. 1994;19(3):532–539. - PubMed
-
- Pan HB, Liang HL, Lin YH, Chung HM, Wu TH, Chen CY, et al. Metallic stent placement for treating peripheral outflow lesions in native arteriovenous fistula hemodialysis patients after insufficient balloon dilatation. AJR Am J Roentgenol. 2005;184(2):403–9. doi: 10.2214/ajr.184.2.01840403. - DOI - PubMed
-
- Stevenson KB, Hannah EL, Lowder CA, Adcox MJ, Davidson RL, Mallea MC, et al. Epidemiology of hemodialysis vascular access infections from longitudinal infection surveillance data: predicting the impact of NKF-DOQI clinical practice guidelines for vascular access. Am J Kidney Dis. 2002;39(3):549–55. doi: 10.1053/ajkd.2002.31405. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources