

Utility of sepsis biomarkers and the infection probability score to discriminate sepsis and systemic inflammatory response syndrome in standard care patients
- PMID: 24349403
- PMCID: PMC3859603
- DOI: 10.1371/journal.pone.0082946
Utility of sepsis biomarkers and the infection probability score to discriminate sepsis and systemic inflammatory response syndrome in standard care patients
Abstract
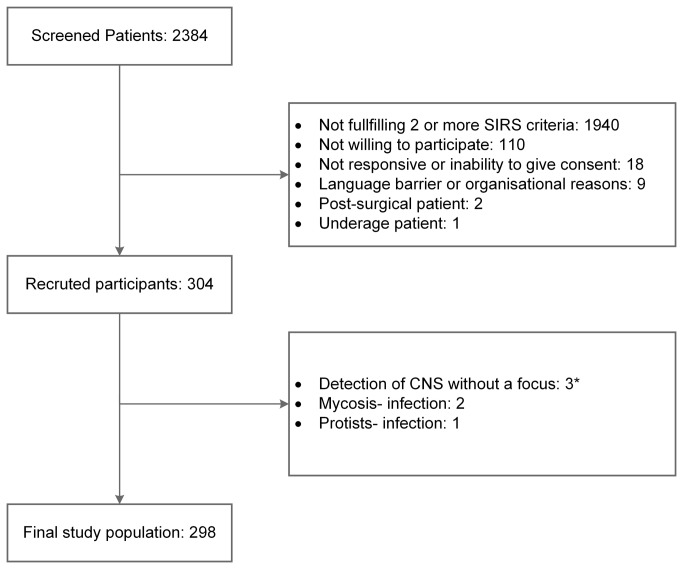
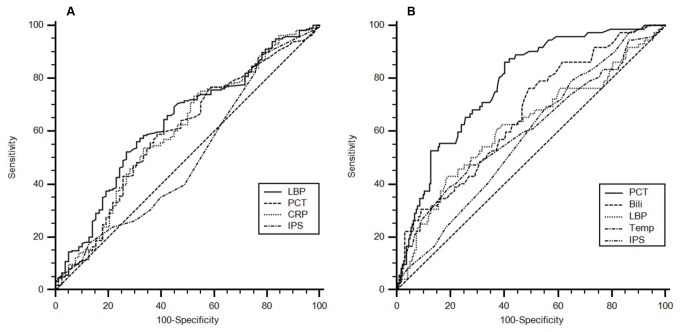
Physicians are regularly faced with severely ill patients at risk of developing infections. In literature, standard care wards are often neglected, although their patients frequently suffer from a systemic inflammatory response syndrome (SIRS) of unknown origin. Fast identification of patients with infections is vital, as they immediately require appropriate therapy. Further, tools with a high negative predictive value (NPV) to exclude infection or bacteremia are important to increase the cost effectiveness of microbiological examinations and to avoid inappropriate antibiotic treatment. In this prospective cohort study, 2,384 patients with suspected infections were screened for suffering from two or more SIRS criteria on standard care wards. The infection probability score (IPS) and sepsis biomarkers with discriminatory power were assessed regarding their capacity to identify infection or bacteremia. In this cohort finally consisting of 298 SIRS-patients, the infection prevalence was 72%. Bacteremia was found in 25% of cases. For the prediction of infection, the IPS yielded 0.51 ROC-AUC (30.1% sensitivity, 64.6% specificity). Among sepsis biomarkers, lipopolysaccharide binding protein (LBP) was the best parameter with 0.63 ROC-AUC (57.5% sensitivity, 67.1% specificity). For the prediction of bacteremia, the IPS performed slightly better with a ROC-AUC of 0.58 (21.3% sensitivity, 65% specificity). Procalcitonin was the best discriminator with 0.78 ROC-AUC, 86.3% sensitivity, 59.6% specificity and 92.9% NPV. Furthermore, bilirubin and LBP (ROC-AUC: 0.65, 0.62) might also be considered as useful parameters. In summary, the IPS and widely used infection parameters, including CRP or WBC, yielded a poor diagnostic performance for the detection of infection or bacteremia. Additional sepsis biomarkers do not aid in discriminating inflammation from infection. For the prediction of bacteremia procalcitonin, and bilirubin were the most promising parameters, which might be used as a rule for when to take blood cultures or using nucleic acid amplification tests for microbiological diagnostics.
Conflict of interest statement
Figures
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, et al. (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101: 1644-1655 - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE et al. (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34: 1589-1596. doi:10.1097/01.CCM.0000217961.75225.E9. PubMed: 16625125. - DOI - PubMed
-
- Davey P, Brown E, Charani E, Fenelon L, Gould IM et al. (2013) Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 4: CD003543. PubMed: 2363331316235326. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
