

A lower level of forced expiratory volume in 1 second is a risk factor for all-cause and cardiovascular mortality in a Japanese population: the Takahata study
- PMID: 24349548
- PMCID: PMC3862812
- DOI: 10.1371/journal.pone.0083725
A lower level of forced expiratory volume in 1 second is a risk factor for all-cause and cardiovascular mortality in a Japanese population: the Takahata study
Abstract
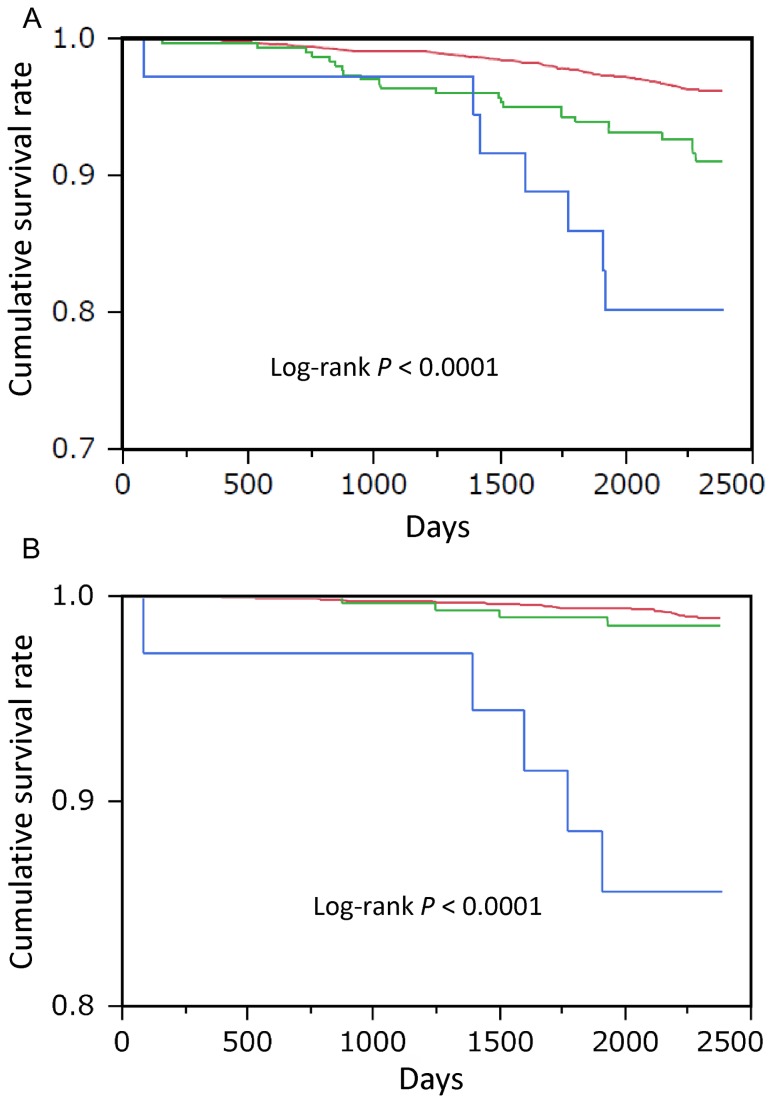
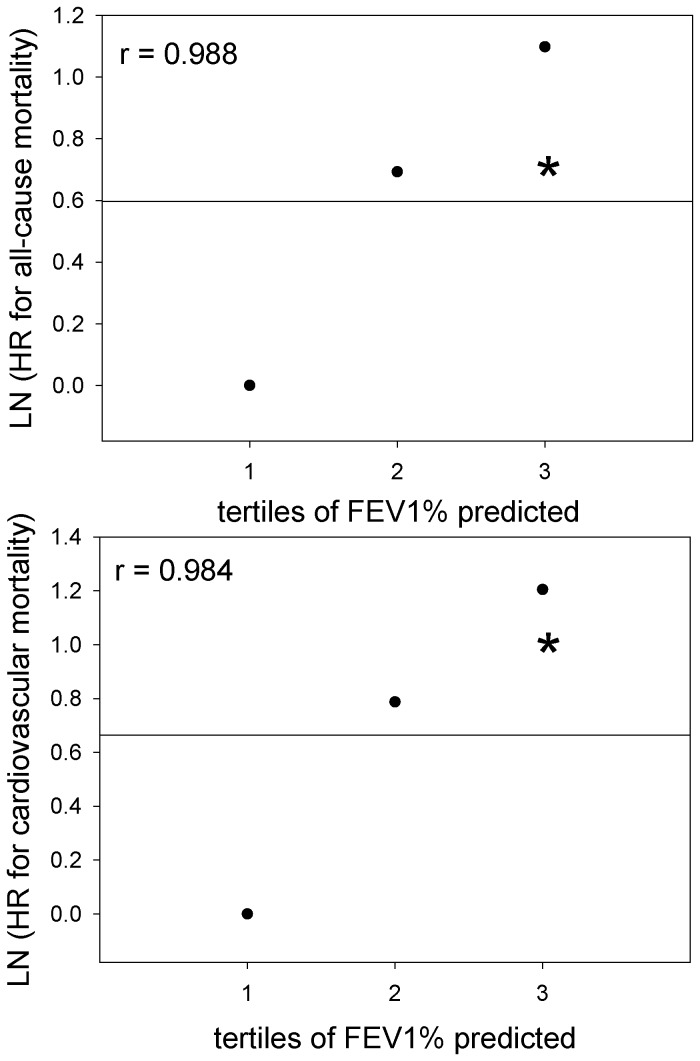
Chronic obstructive pulmonary disease is a known risk factor for cardiovascular death in Western countries. Because Japan has a low cardiovascular death rate, the association between a lower level of forced expiratory volume in 1 s (FEV1) and mortality in Japan's general population is unknown. To clarify this, we conducted a community-based longitudinal study. This study included 3253 subjects, who received spirometry from 2004 to 2006 in Takahata, with a 7-year follow-up. The causes of death were assessed on the basis of the death certificate. In 338 subjects, airflow obstruction was observed by spirometry. A total of 127 subjects died. Cardiovascular death was the second highest cause of death in this population. The pulmonary functions of the deceased subjects were significantly lower than those of the subjects who were alive at the end of follow-up. The relative risk of death by all causes, respiratory failure, lung cancer, and cardiovascular disease was significantly increased with airflow obstruction. The Kaplan-Meier analysis showed that all-cause and cardiovascular mortality significantly increased with a worsening severity of airflow obstruction. After adjusting for possible factors that could influence prognosis, a Cox proportional hazard model analysis revealed that a lower level of FEV1 was an independent risk factor for all-cause and cardiovascular mortality (per 10% increase; hazard ratio [HR], 0.89; 95% confidence interval [CI], 0.82-0.98; and HR, 0.72; 95% CI, 0.61-0.86, respectively). In conclusion, airflow obstruction is an independent risk factor for all-cause and cardiovascular death in the Japanese general population. Spirometry might be a useful test to evaluate the risk of cardiovascular death and detect the risk of respiratory death by lung cancer or respiratory failure in healthy Japanese individuals.
Conflict of interest statement
Figures
References
-
- GOLD Global Initiative for Chronic. Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (updated 2011). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
