

Rare myeloid sarcoma/acute myeloid leukemia with adrenal mass after allogeneic mobilization peripheral blood stem cell transplantation
- PMID: 24349834
- PMCID: PMC3860347
- DOI: 10.7497/j.issn.2095-3941.2013.04.008
Rare myeloid sarcoma/acute myeloid leukemia with adrenal mass after allogeneic mobilization peripheral blood stem cell transplantation
Abstract
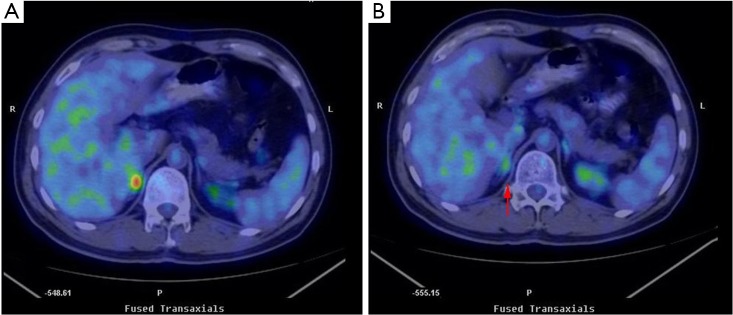
Myeloid sarcoma (MS) is a rare hematological neoplasm that develops either de novo or concurrently with acute myeloid leukemia (AML). This neoplasm can also be an initial manifestation of relapse in a previously treated AML that is in remission. A 44-year-old male patient was diagnosed with testis MS in a local hospital in August 2010. After one month, bone marrow biopsy and aspiration confirmed the diagnosis of AML. Allogeneic mobilization peripheral blood stem cell transplantation was performed, with the sister of the patient as donor, after complete remission (CR) was achieved by chemotherapy. Five months after treatment, an adrenal mass was detected by positron emission tomography-computed tomography (PET-CT). Radiotherapy was performed for the localized mass after a multidisciplinary team (MDT) discussion. The patient is still alive as of May 2013, with no evidence of recurrent MS or leukemia.
Keywords: Myeloid sarcoma (MS); acute myeloid leukemia (AML); allogeneic hematopoietic stem cell transplantation; multidisciplinary team (MDT).
Conflict of interest statement
No potential conflicts of interest are disclosed.
Figures
Similar articles
-
Myeloid Sarcoma of the Paranasal Sinuses in a Patient with Acute Myeloid Leukemia.Tohoku J Exp Med. 2018 Oct;246(2):141-146. doi: 10.1620/tjem.246.141. Tohoku J Exp Med. 2018. PMID: 30369515
-
Clinical outcome of myeloid sarcoma in adult patients and effect of allogeneic stem cell transplantation. Results from a multicenter survey.Leuk Res. 2017 Feb;53:74-81. doi: 10.1016/j.leukres.2016.12.003. Epub 2016 Dec 20. Leuk Res. 2017. PMID: 28056398
-
Relapsed acute myeloid leukemia presenting as conjunctival myeloid sarcoma: a case report.BMC Ophthalmol. 2022 Feb 10;22(1):65. doi: 10.1186/s12886-022-02286-1. BMC Ophthalmol. 2022. PMID: 35144564 Free PMC article.
-
Vulvar myeloid sarcoma as the presenting symptom of acute myeloid leukemia: a case report and literature review of Chinese patients, 1999-2018.Diagn Pathol. 2019 Nov 7;14(1):126. doi: 10.1186/s13000-019-0892-3. Diagn Pathol. 2019. PMID: 31699112 Free PMC article. Review.
-
Extramedullary tumors of myeloid blasts in adults as a pattern of relapse following allogeneic bone marrow transplantation.Cancer. 1999 Feb 1;85(3):608-15. doi: 10.1002/(sici)1097-0142(19990201)85:3<608::aid-cncr11>3.0.co;2-5. Cancer. 1999. PMID: 10091734 Review.
Cited by
-
Immunohistochemical Biomarkers in Diagnosis of Hematolymphoid Neoplasms of Endocrine Organs.Endocr Pathol. 2018 Jun;29(2):176-188. doi: 10.1007/s12022-018-9533-8. Endocr Pathol. 2018. PMID: 29855797 Free PMC article. Review.
-
The progression of CD56+ myeloid sarcoma: A case report and literature review.Oncol Lett. 2016 May;11(5):3091-3096. doi: 10.3892/ol.2016.4352. Epub 2016 Mar 18. Oncol Lett. 2016. PMID: 27123069 Free PMC article.
References
-
- Klco JM, Welch JS, Nguyen TT, Hurley MY, Kreisel FH, Hassan A, et al. State of the art in myeloid sarcoma. Int J Lab Hematol 2011;33:555-565 - PubMed
-
- Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M, et al. Myeloid sarcoma: clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia 2007;21:340-350 - PubMed
-
- The International Agency for Research on Cancer eds. (2008) WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue. IARC Press, Lyon, 2008;140-141.
-
- NCCN Clinical Practice Guidelines in Oncology: Acute Myeloid Leukemia, Version 2. 2012.
-
- Low G, Dhliwayo H, Lomas DJ. Adrenal neoplasms. Clin Radiol 2012;67:988-1000 - PubMed
Publication types
LinkOut - more resources
Full Text Sources