

Time of admission, gender and age: challenging factors in emergency renal colic - a preliminary study
- PMID: 24350118
- PMCID: PMC3860620
- DOI: 10.5812/traumamon.6800
Time of admission, gender and age: challenging factors in emergency renal colic - a preliminary study
Abstract
Background: Nephrolithiasis is a relatively common problem and a frequent Emergency Department (ED) diagnosis in patients who present with acute flank/abdominal pain. The pain management in these patients is often challenging.
Objectives: To investigate the most effective dose of morphine with the least side effects in emergency renal colic patients.
Materials and methods: 150 renal colic patients who experienced a pain level of 4 or greater, based on visual analog scale (VAS) at admission time were included. Pain was scored on a 100 mm VAS (0 = no pain, 100 = the worst pain imagined). When patients arrived at ED, a physician would examine the patients and assessed initial pain score, then filled a questionnaire according to the patient information. Patients were assigned to receive 2.5 mg morphine sulfate intravenously. We monitored patients' visual analog scale (VAS), and adverse events at different time points (every 15 minutes) for 90 minutes. Additional doses of intravenous morphine (2.5 mg) were administered if the patient still had pain. (Max dose: 10 mg). The cumulative dose of morphine, defined as the total amount of morphine prescribed to each patient during the 90 minutes of the study, was recorded. Patients were not permitted to use any nonsteroidal anti-inflammatory drugs as coadjuvant analgesics during the study period. Subjects with inadequate pain relief at 90 minutes received rescue morphine and were excluded from the study. The primary end point in this study was pain relief at 90 minutes, defined as either VAS<40 or decrease of 50% or more as compared to the initial VAS. The secondary objective was to detect the occurrence of adverse effects at any time points in ED.
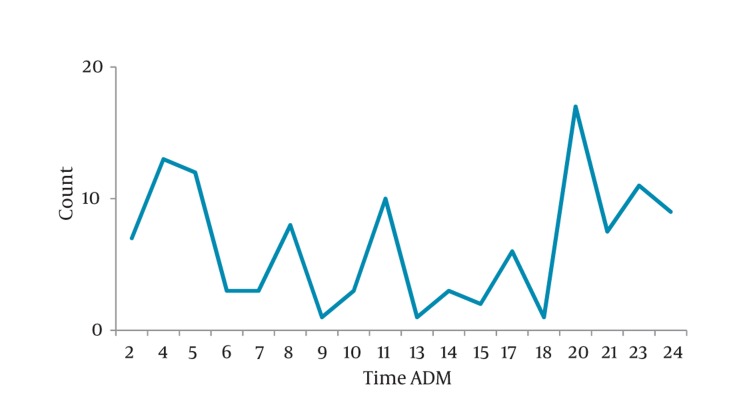
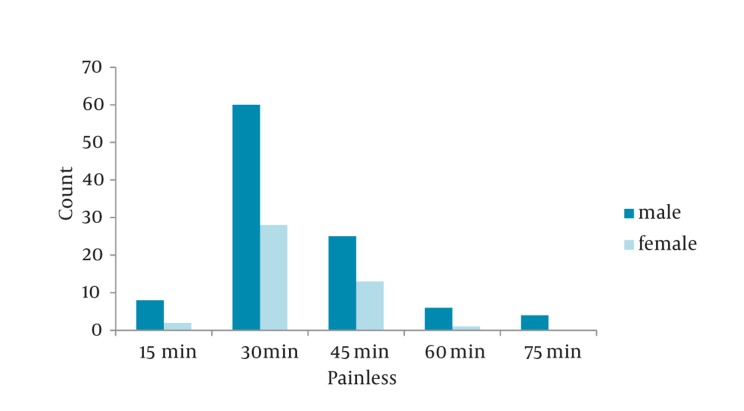
Results: The studied patients consisted of 104 men and 46 women with the mean age of 43 ±14 years (range, 18 to 75 years). There was no statistically significant difference between the mean age and gender differences in pain response. Rescue analgesia at 30 minutes were given in 54.5% receiving morphine. The average time to painless was 35 minutes. But there were no statistically significant differences between the mean age and gender differences in pain response (P > 0.05). Older patients responded sooner to morphine than the young. Most of the patients had a pain score of 90 -100 (77.3 %) at the beginning that was reduced to 29.4% during the 30 minutes follow up. During the first hour, we found that 94.7% of the patients had no pain or significant pain reduction and only 2.1% of the patients still had pain.
Conclusions: We conclude that there were no significant differences among the gender, time of admission and side - effects in renal colic patients in response to morphine.
Keywords: Adverse Effect; Gender; Morphine; Renal Colic.
Figures


References
-
- Morgan S. Intravenous paracetamol in patients with renal colic. Emerg Nurse. 2011;18(9):22–5. - PubMed
-
- Steinberg PL, Nangia AK, Curtis K. A standardized pain management protocol improves timeliness of analgesia among emergency department patients with renal colic. Qual Manag Health Care. 2011;20(1):30–6. - PubMed
LinkOut - more resources
Full Text Sources
Medical