

Magnesium sulphate for fetal neuroprotection: a cost-effectiveness analysis
- PMID: 24350635
- PMCID: PMC3878233
- DOI: 10.1186/1472-6963-13-527
Magnesium sulphate for fetal neuroprotection: a cost-effectiveness analysis
Abstract
Background: The aim of this study was to assess the cost-effectiveness of administering magnesium sulphate to patients in whom preterm birth at < 32+0 weeks gestation is either imminent or threatened for the purpose of fetal neuroprotection.
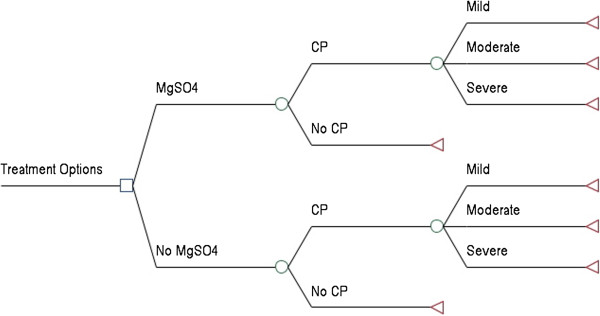
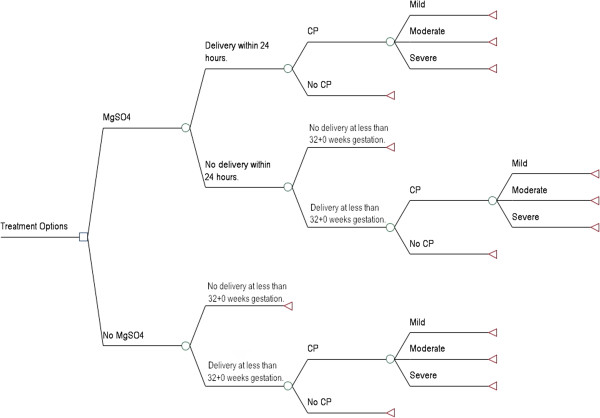
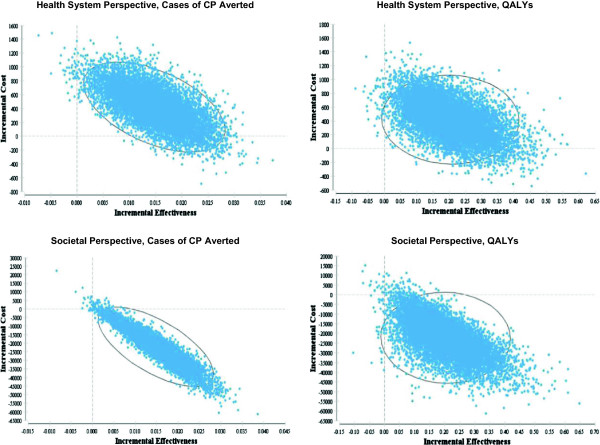
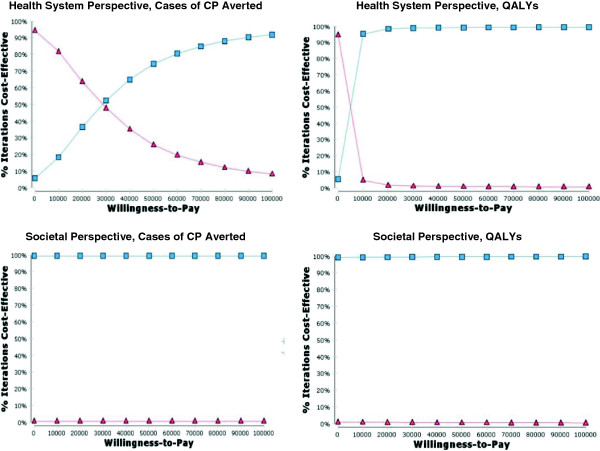
Methods: Multiple decision tree models and probabilistic sensitivity analyses were used to compare the administration of magnesium sulphate with the alternative of no treatment. Two separate cost perspectives were utilized in this series of analyses: a health system and a societal perspective. In addition, two separate measures of effectiveness were utilized: cases of cerebral palsy (CP) averted and quality-adjusted life years (QALYs).
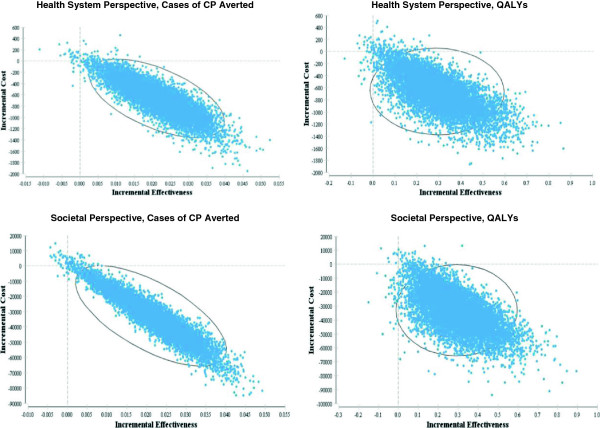
Results: From a health system and a societal perspective, respectively, a savings of $2,242 and $112,602 is obtained for each QALY gained and a savings of $30,942 and $1,554,198 is obtained for each case of CP averted when magnesium sulphate is administered to patients in whom preterm birth is imminent. From a health system perspective and a societal perspective, respectively, a cost of $2,083 is incurred and a savings of $108,277 is obtained for each QALY gained and a cost of $28,755 is incurred and a savings of $1,494,500 is obtained for each case of CP averted when magnesium sulphate is administered to patients in whom preterm birth is threatened.
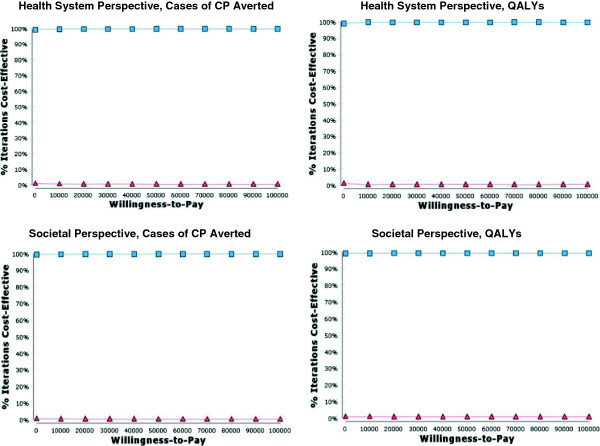
Conclusions: Administration of magnesium sulphate to patients in whom preterm birth is imminent is a dominant (i.e. cost-effective) strategy, no matter what cost perspective or measure of effectiveness is used. Administration of magnesium sulphate to patients in whom preterm birth is threatened is a dominant strategy from a societal perspective and is very likely to be cost-effective from a health system perspective.
Figures
References
-
- Kruse M, Michelsen SI, Flachs EM, Brønnum-Hansen H, Madsen M, Uldall P. Lifetime costs of cerebral palsy. Dev Med Child Neurol. 2009;13:622–628. - PubMed
-
- Rosenbaum PL, Livingston MH, Palisano RJ, Galuppi BE, Russell DJ. Quality of life and health-related quality of life of adolescents with cerebral palsy. Dev Med Child Neurol. 2007;13:516–521. - PubMed
-
- Young NL, Rochon TG, McCormick A, Law M, Wedge JH, Fehlings D. The health and quality of life outcomes among youth and young adults with cerebral palsy. Arch Phys Med Rehabil. 2010;13:143–148. - PubMed
-
- Drummond PM, Colver AF. Analysis by gestational age of cerebral palsy in singleton births in north-east England 1970–94. Paediatr Perinat Epidemiol. 2002;13:172–180. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
