

Engineering muscle constructs for the creation of functional engineered musculoskeletal tissue
- PMID: 24351009
- PMCID: PMC4482104
- DOI: 10.2217/rme.13.81
Engineering muscle constructs for the creation of functional engineered musculoskeletal tissue
Abstract
Volumetric muscle loss (VML) is a disabling condition in which current clinical procedures are suboptimal. The field of tissue engineering has many promising strategies for the creation of functional skeletal muscle in vitro. However, there are still two key limitations that prevent it from becoming a solution for treating VML. First, engineered muscle tissue must be biocompatible to facilitate muscle tissue regrowth without generating an immune response. Second, engineered muscle constructs must be scaled up to facilitate replacement of clinically relevant volumes of tissue (centimeters in diameter). There are currently no tissue engineering strategies to produce tissue constructs that are both biocompatible and large enough to facilitate clinical repair. However, recent advances in tissue engineering using synthetic scaffolds, native scaffolds, or scaffold-free approaches may lead to a solution for repair of VML injuries.
Figures

References
-
- Vandenburgh HH, Karlisch P, Farr L. Maintenance of highly contractile tissue-cultured avian skeletal myotubes in collagen gel. In Vitro Cell. Dev. Biol. 1988;24(3):166–174. - PubMed
-
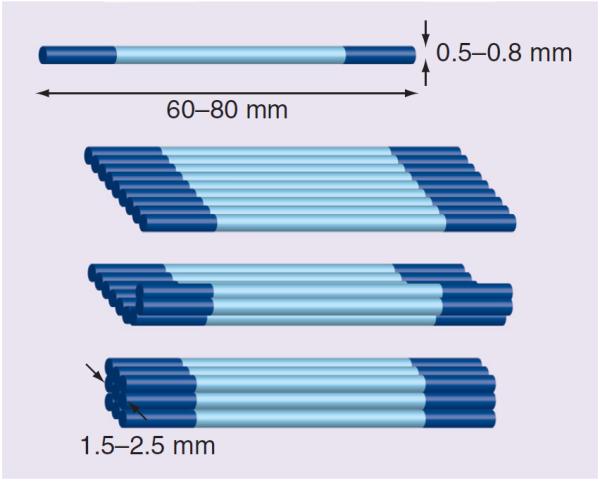
- Page RL, Malcuit C, Vilner L, et al. Restoration of skeletal muscle defects with adult human cells delivered on fibrin microthreads. Tissue Eng. Part A. 2011;17(21–22):2629–2640. - PubMed
-
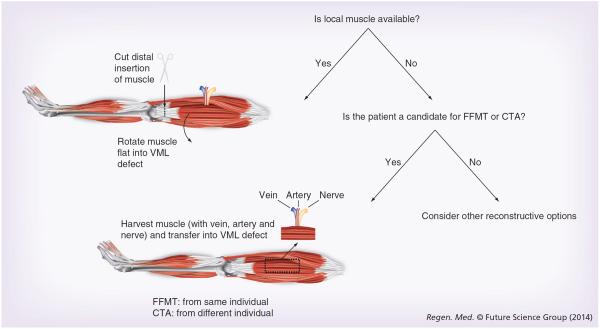
- Chuang D. Free tissue transfer for the treatment of facial paralysis. Facial Plast. Surg. 2008;24(2):194–203. - PubMed
-
- Koning M, Harmsen MC, van Luyn MJA, Werker PMN. Current opportunities and challenges in skeletal muscle tissue engineering. J. Tissue Eng. Regen. Med. 2009;3(6):407–415. - PubMed
-
■■ Discusses the current challenges faced by skeletal muscle tissue engineering technologies and gives a concise review of the current state of the art in tissue engineering of skeletal muscle and the opportunities and challenges for future clinical applicability.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources