

The evidence base for diabetes technology: appropriate and inappropriate meta-analysis
- PMID: 24351183
- PMCID: PMC3876335
- DOI: 10.1177/193229681300700617
The evidence base for diabetes technology: appropriate and inappropriate meta-analysis
Abstract
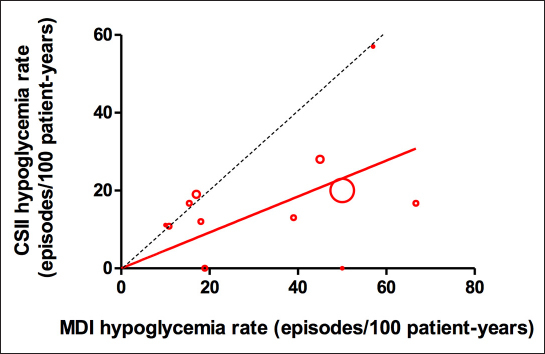
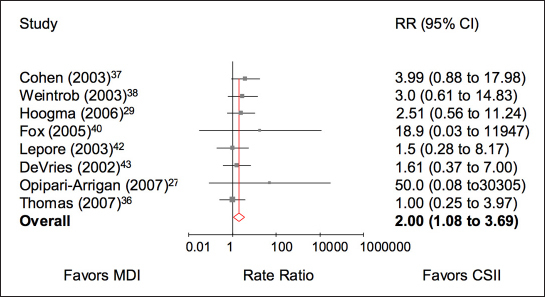
When we are interested in making decisions about best use, comparative therapeutic efficacy, or cost-effectiveness of diabetes technologies such as insulin pump therapy [continuous subcutaneous insulin infusion (CSII)] or continuous glucose monitoring, meta-analysis for the purpose of literature summary is inappropriate and may be misleading. Instead, "decision-making meta-analysis" is more appropriate and should involve either preselection of trials based on intended use [e.g., elevated baseline hemoglobin A1c or hypoglycemia rate for trials of multiple daily injections (MDI) versus CSII] or metaregression of summary effect sizes in different trials against potential effect-modifying covariates such as baseline risk, or models of the covariates that determine effect size using individual patient data. Appropriate meta-analysis should also only include trials that are of sufficient duration to accurately measure outcomes such as severe hypoglycemia, and they should not use obsolete technology that is of proven inferiority to current technology. The use of appropriate decision-making meta-analysis is illustrated by the change in the rate ratio for severe hypoglycemia in randomized controlled trials of MDI versus CSII in type 1 diabetes from 1.56 (95% confidence interval 0.96-2.55; p = .074) for literature-summary meta-analysis to 2.0 (1.08-3.69; p = .027) for decision-making meta-analysis of all patients and 3.91 (1.35-11.36; p = .01) for trials in children.
© 2013 Diabetes Technology Society.
Figures

References
-
- National Institute for Health and Care Excellence. Guide to the methods of technology appraisal. 2013. http://publications.nice.org.uk/pmg9. Accessed April 9, 2013. - PubMed
-
- Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control in Type 1 diabetes: meta-analysis of multiple daily insulin injections compared with continuous subcutaneous insulin infusion. Diabet Med. 2008;25(7):765–774. - PubMed
-
- Fatourechi MM, Kudva YC, Murad MH, Elamin MB, Tabini CC, Montori VM. Clinical review: Hypoglycemia with intensive insulin therapy: a systematic review and meta-analyses of randomized trials of continuous subcutaneous insulin infusion versus multiple daily injections. J Clin Endocrinol Metab. 2009;94(3):729–740. - PubMed
-
- Pankowska E, Blazik M, Dziechciarz P, Szypowska A, Szajewska H. Continuous subcutaneous insulin infusion vs. multiple daily injections in children with type 1 diabetes: a systematic review and meta-analysis of randomized control trials. Pediatr Diabetes. 2009;10(1):52–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
