

Effects of conventional therapeutic interventions on the number and function of regulatory T cells
- PMID: 24353914
- PMCID: PMC3862634
- DOI: 10.4161/onci.27025
Effects of conventional therapeutic interventions on the number and function of regulatory T cells
Abstract
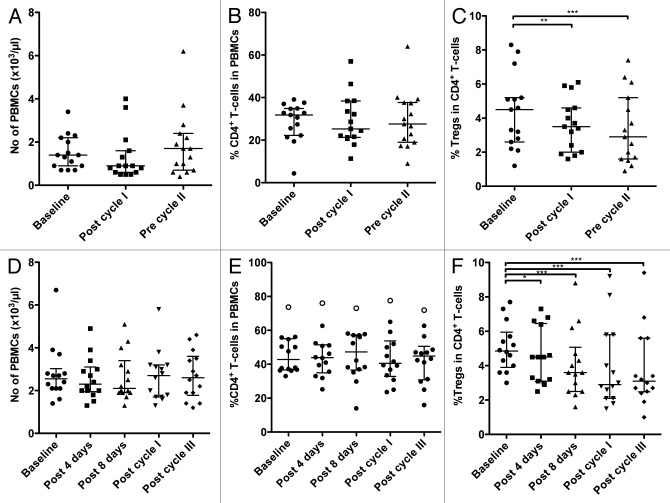
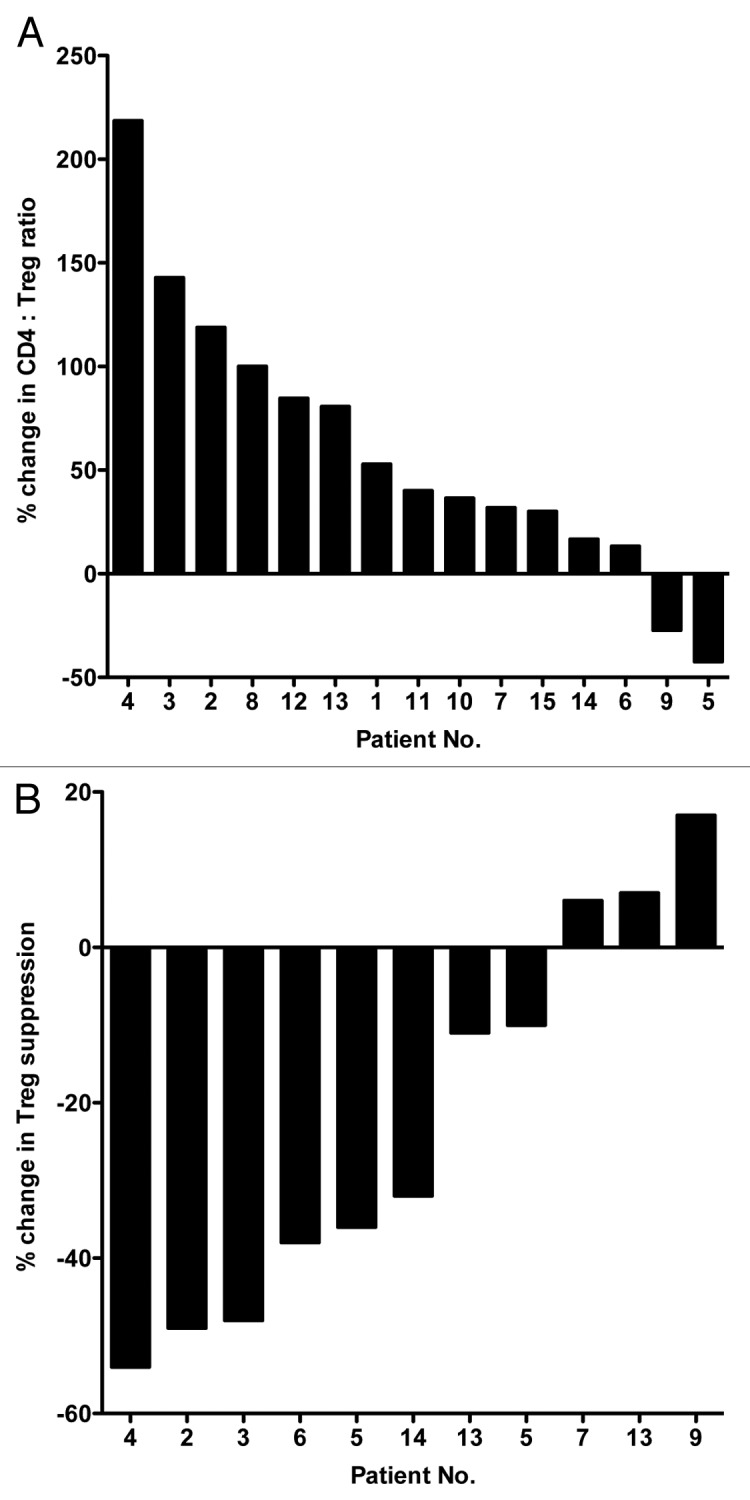
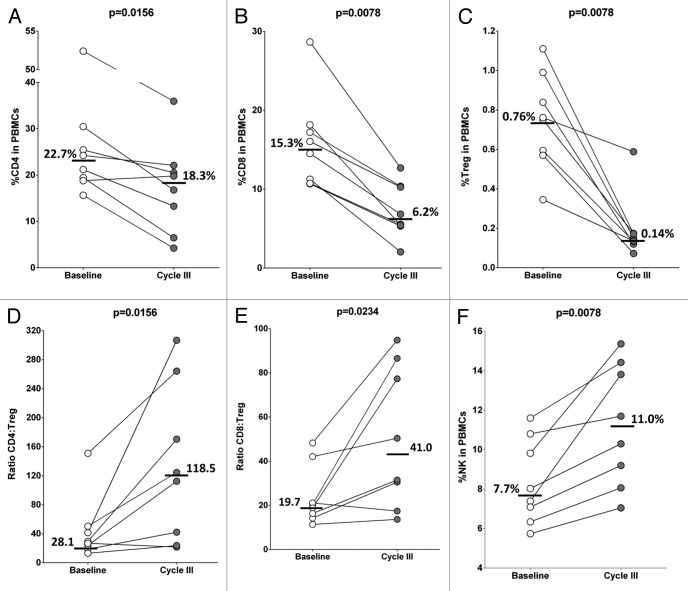
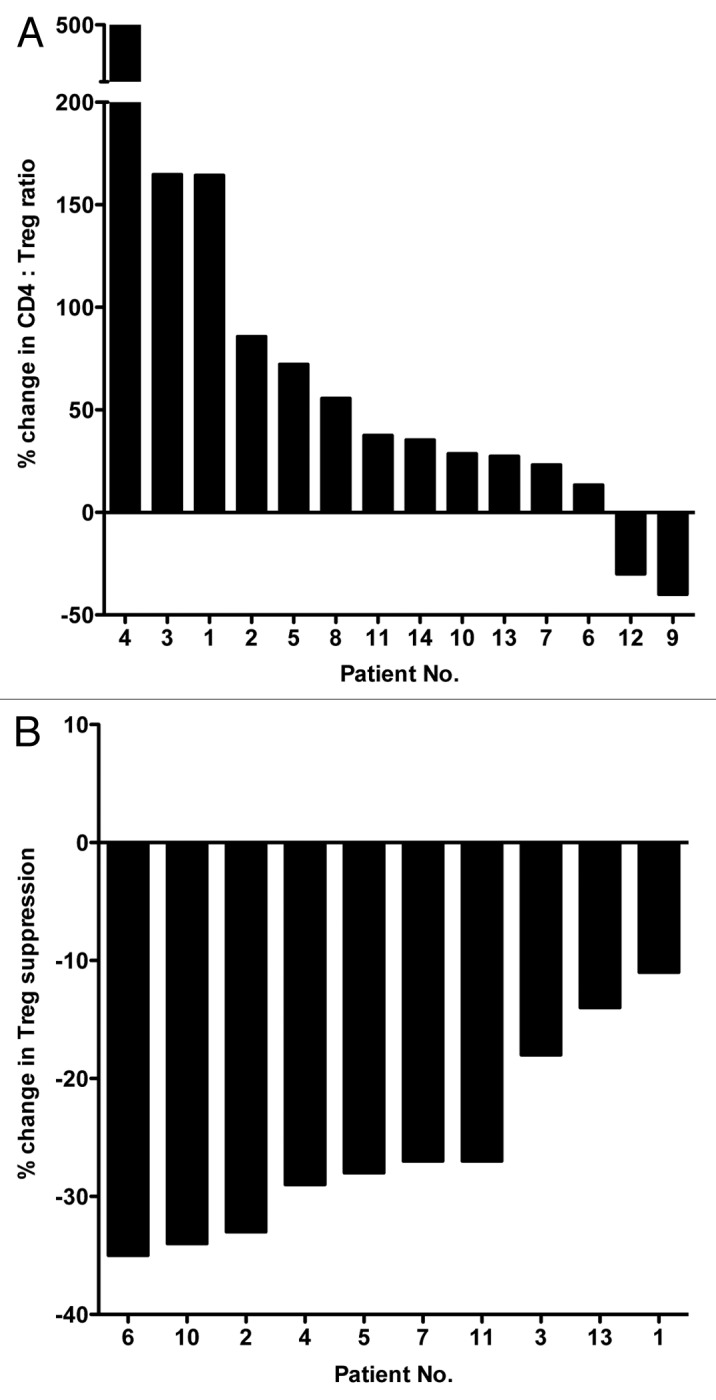
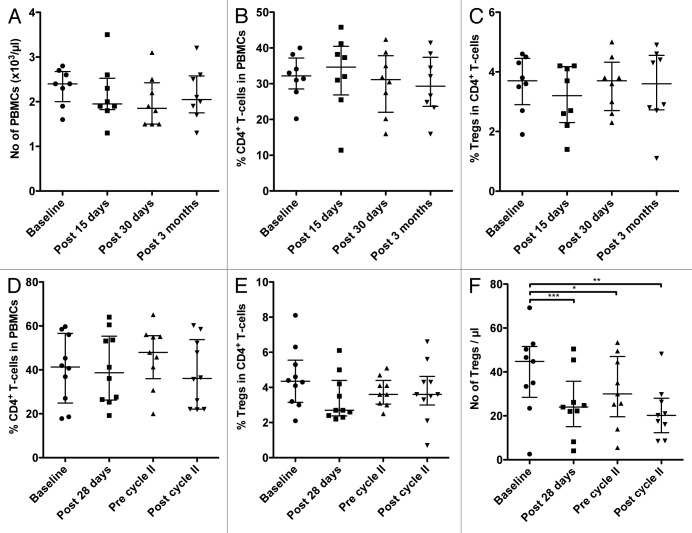
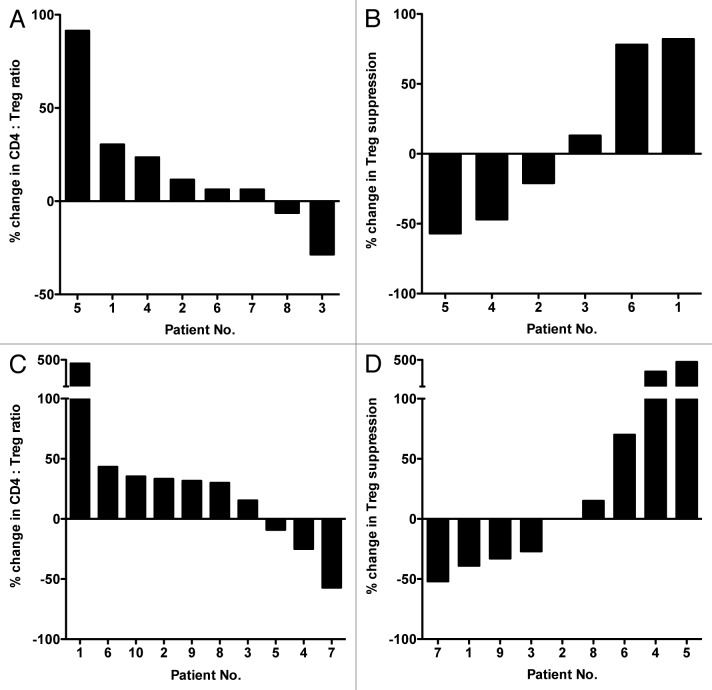
Several lines of investigation have revealed the apparent interplay between the immune system of the host and many conventional, "standard-of-care" anticancer therapies, including chemotherapy and small molecule targeted therapeutics. In particular, preclinical and clinical studies have demonstrated the important role of regulatory T cells (Tregs) in inhibiting immune responses elicited by immunotherapeutic regimens such as those based on anticancer vaccines or checkpoint inhibitors. However, how the number and immunosuppressive function of Tregs change in cancer patients undergoing treatment with non-immune anticancer therapies remains to be precisely elucidated. To determine whether immunostimulatory therapies can be employed successfully in combination with conventional anticancer regimens, we have investigated both the number and function of Tregs obtained from the peripheral blood of carcinoma patients before the initiation and during the course of chemotherapeutic and targeted agent regimens. Our studies show that the treatment of breast cancer patients with tamoxifen plus leuprolide, a gonadotropin releasing hormone agonist, has minimal effects on Tregs, while sunitinib appears to exert differential effects on Tregs among patients with metastatic renal carcinoma. However, the administration of docetaxel to patients with metastatic prostate or breast cancer, as well as that of cisplatin plus vinorelbine to non-small cell lung cancer patients, appears to significantly increase the ratio between effector T cells and Tregs and to reduce the immunosuppressive activity of the latter in the majority of patients. These studies provide the rationale for the selective use of active immunotherapy regimens in combination with specific standard-of-care therapies to achieve the most beneficial clinical outcome among carcinoma patients.
Keywords: T lymphocytes; Tregs; carcinoma; chemotherapy; drug therapy.
Figures
Similar articles
-
Recent strategies for the use of paclitaxel in the treatment of urological malignancies.World J Urol. 1998;16(2):155-62. doi: 10.1007/s003450050044. World J Urol. 1998. PMID: 12073232 Review.
-
Immune modulations during chemoimmunotherapy & novel vaccine strategies--in metastatic melanoma and non small-cell lung cancer.Dan Med J. 2013 Dec;60(12):B4774. Dan Med J. 2013. PMID: 24355457 Review.
-
Expression of costimulatory and inhibitory receptors in FoxP3+ regulatory T cells within the tumor microenvironment: Implications for combination immunotherapy approaches.Adv Cancer Res. 2019;144:193-261. doi: 10.1016/bs.acr.2019.05.001. Epub 2019 Jun 6. Adv Cancer Res. 2019. PMID: 31349899 Review.
-
The Impact of Tregs on the Anticancer Immunity and the Efficacy of Immune Checkpoint Inhibitor Therapies.Front Immunol. 2021 Feb 26;12:625783. doi: 10.3389/fimmu.2021.625783. eCollection 2021. Front Immunol. 2021. PMID: 33717139 Free PMC article. Review.
-
The association of clinical outcome and peripheral T-cell subsets in metastatic colorectal cancer patients receiving first-line FOLFIRI plus bevacizumab therapy.Oncoimmunology. 2016 May 19;5(7):e1188243. doi: 10.1080/2162402X.2016.1188243. eCollection 2016 Jul. Oncoimmunology. 2016. PMID: 27622042 Free PMC article.
Cited by
-
Hyperprogressive disease with immunotherapy: new directions.J Thorac Dis. 2019 Sep;11(Suppl 15):S1877-S1880. doi: 10.21037/jtd.2019.08.88. J Thorac Dis. 2019. PMID: 31632773 Free PMC article. No abstract available.
-
Wnt/β-Catenin Signaling and Resistance to Immune Checkpoint Inhibitors: From Non-Small-Cell Lung Cancer to Other Cancers.Biomedicines. 2023 Jan 12;11(1):190. doi: 10.3390/biomedicines11010190. Biomedicines. 2023. PMID: 36672698 Free PMC article. Review.
-
Post-progression survival after cessation of treatment with nivolumab for advanced non-small cell lung cancer: A retrospective study.PLoS One. 2018 Aug 28;13(8):e0203070. doi: 10.1371/journal.pone.0203070. eCollection 2018. PLoS One. 2018. PMID: 30153300 Free PMC article.
-
JME-001 phase II trial of first-line combination chemotherapy with cisplatin, pemetrexed, and nivolumab for unresectable malignant pleural mesothelioma.J Immunother Cancer. 2021 Oct;9(10):e003288. doi: 10.1136/jitc-2021-003288. J Immunother Cancer. 2021. PMID: 34711664 Free PMC article. Clinical Trial.
-
Immunotherapy for Non-small Cell Lung Cancer: Current Landscape and Future Perspectives.Immune Netw. 2020 Jan 27;20(1):e10. doi: 10.4110/in.2020.20.e10. eCollection 2020 Feb. Immune Netw. 2020. PMID: 32158598 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical