

High-grade adult isthmic L5-s1 spondylolisthesis: a report of intraoperative slip progression treated with surgical reduction and posterior instrumented fusion
- PMID: 24353957
- PMCID: PMC3864463
- DOI: 10.1055/s-0032-1307257
High-grade adult isthmic L5-s1 spondylolisthesis: a report of intraoperative slip progression treated with surgical reduction and posterior instrumented fusion
Abstract
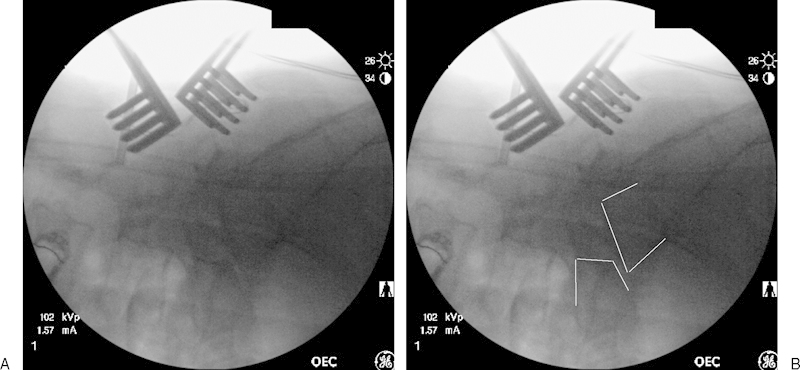
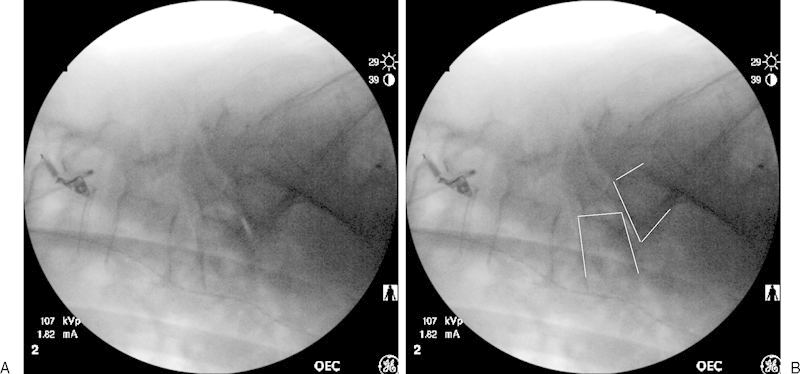
Adult isthmic spondylolisthesis most commonly occurs at the L5-S1 level of the lumbar spine. Slip progression is relatively rare in adults with this condition and slippage is typically associated with advanced degeneration of the disk below the pars defect. When symptomatic, radiculopathy is the typical complaint in adults with isthmic spondylolisthesis. When considering options for surgical treatment of adult isthmic spondylolisthesis, the surgeon must consider several different options, such as decompression, fusion, instrumentation, reduction, and type of bone graft to be used. All of these decisions must be individualized as deemed appropriate for each particular patient. This report presents a case of intraoperative slip progression of a L5-S1 adult isthmic spondylolisthesis to a high-grade slip, which was treated with complete surgical reduction and posterior instrumented fusion. This case demonstrates the potential instability of this condition in adults and has not been previously reported. The case details and images are reviewed and the intraoperative decisions, treatment options, and patient outcome are discussed.
Keywords: adult isthmic spondylolisthesis; high-grade spondylolisthesis; posterior instrumented fusion; slip progression; surgical reduction.
Figures




Similar articles
-
Transvertebral Transsacral strut grafting for high-grade isthmic spondylolisthesis L5-S1 with fibular allograft.J Spinal Disord Tech. 2008 Jul;21(5):328-33. doi: 10.1097/BSD.0b013e318149e7ea. J Spinal Disord Tech. 2008. PMID: 18600142
-
[Adjacent segment degeneration after lumbosacral fusion in spondylolisthesis: a retrospective radiological and clinical analysis].Acta Chir Orthop Traumatol Cech. 2010 Apr;77(2):124-30. Acta Chir Orthop Traumatol Cech. 2010. PMID: 20447355 Czech.
-
Instrumented slip reduction and fusion for painful unstable isthmic spondylolisthesis in adults.J Spinal Disord Tech. 2008 Oct;21(7):477-83. doi: 10.1097/BSD.0b013e31815b1abf. J Spinal Disord Tech. 2008. PMID: 18836358
-
Acute progression of spondylolysis to isthmic spondylolisthesis in an adult.Spine (Phila Pa 1976). 2002 Aug 15;27(16):E370-2. doi: 10.1097/00007632-200208150-00023. Spine (Phila Pa 1976). 2002. PMID: 12195078 Review.
-
Is Stand-Alone Anterior Lumbar Interbody Fusion a Safe and Efficacious Treatment for Isthmic Spondylolisthesis of L5-S1?Global Spine J. 2017 Sep;7(6):587-595. doi: 10.1177/2192568217699210. Epub 2017 Jun 1. Global Spine J. 2017. PMID: 28894689 Free PMC article. Review.
Cited by
-
Short- and Mid-Term Outcomes Following ALIF and TLIF in L5-S1 Isthmic Spondylolisthesis Patients.Int J Spine Surg. 2025 Mar 6;19(1):81-87. doi: 10.14444/8696. Int J Spine Surg. 2025. PMID: 39805707 Free PMC article.
References
-
- Fredrickson B E, Baker D, McHolick W J, Yuan H A, Lubicky J P. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am. 1984;66:699–707. - PubMed
-
- Meyerding H W. Spondylolisthesis. J Bone Joint Surg Am. 1931;13:39–48.
-
- Wiltse L L, Newman P H, Macnab I. Classification of spondylolisis and spondylolisthesis. Clin Orthop Relat Res. 1976;117:23–29. - PubMed
-
- Farfan H F, Osteria V, Lamy C. The mechanical etiology of spondylolysis and spondylolisthesis. Clin Orthop Relat Res. 1976;117:40–55. - PubMed
-
- Marchetti P C, Bartolozzi P. Philadelphia: Lippincott-Raven; 1997. Classification of spondylolisthesis as a guideline for treatment; pp. 1211–1254.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
