

Association between birthplace and current asthma: the role of environment and acculturation
- PMID: 24354818
- PMCID: PMC4011106
- DOI: 10.2105/AJPH.2013.301509
Association between birthplace and current asthma: the role of environment and acculturation
Abstract
Objectives: We evaluated associations between current asthma and birthplace among major racial/ethnic groups in the United States.
Methods: We used multivariate logistic regression methods to analyze data on 102,524 children and adolescents and 255,156 adults in the National Health Interview Survey (2001-2009).
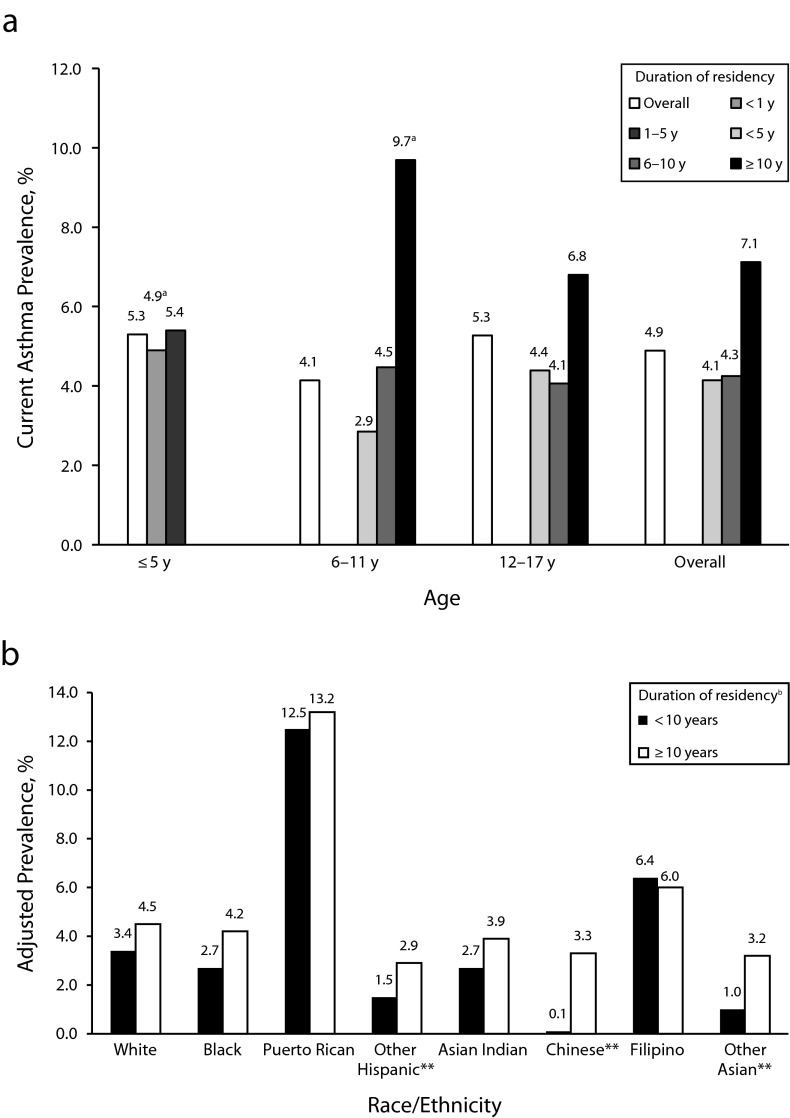
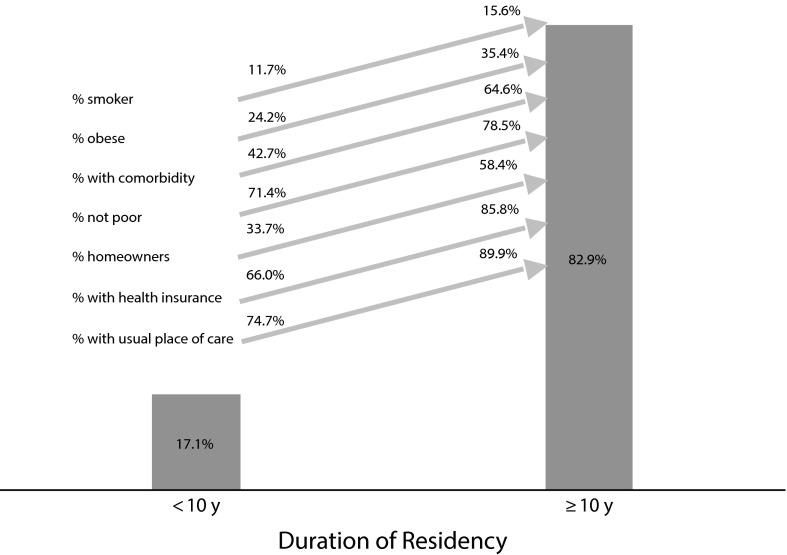
Results: We found significantly higher prevalence (P < .05) of current asthma among children and adolescents (9.3% vs 5.1%) and adults (7.6% vs 4.7%) born in the 50 states and Washington, DC (US-born), than among those born elsewhere. These differences were among all age groups of non-Hispanic Whites, non-Hispanic Blacks, and Hispanics (excluding Puerto Ricans) and among Chinese adults. Non-US-born adults with 10 or more years of residency in the United States had higher odds of current asthma (odds ratio = 1.55; 95% confidence interval = 1.25, 1.93) than did those who arrived more recently. Findings suggested a similar trend among non-US-born children.
Conclusions: Current asthma status was positively associated with being born in the United States and with duration of residency in the United States. Among other contributing factors, changes in environment and acculturation may explain some of the differences in asthma prevalence.
Figures

References
-
- Braman SS. The global burden of asthma. Chest. 2006;130(1 suppl):4S–12S. - PubMed
-
- Mannino DM, Homa DM, Akinbami LJ, Moorman JE, Gwynn C, Redd SC. Surveillance for asthma—United States, 1980–1999. MMWR Surveill Summ. 2002;51(1):1–13. - PubMed
-
- Centers for Disease Control and Prevention. Vital signs: asthma prevalence, disease characteristics, and self-management education—United States, 2001–2009. MMWR Morb Mortal Wkly Rep. 2011;60(17):547–552. - PubMed
-
- Holguin F, Mannino DM, Antó J et al. Country of birth as a risk factor for asthma among Mexican Americans. Am J Respir Crit Care Med. 2005;171(2):103–108. - PubMed
-
- Sundquist J, Winkleby MA. Country of birth, acculturation status and abdominal obesity in a national sample of Mexican-American women and men. Int J Epidemiol. 2000;29(3):470–477. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
