

Endovascular exclusion of the anterior communicating artery with flow-diverter stents as an emergency treatment for blister-like intracranial aneurysms. A case report
- PMID: 24355152
- PMCID: PMC3902747
- DOI: 10.1177/159101991301900411
Endovascular exclusion of the anterior communicating artery with flow-diverter stents as an emergency treatment for blister-like intracranial aneurysms. A case report
Abstract
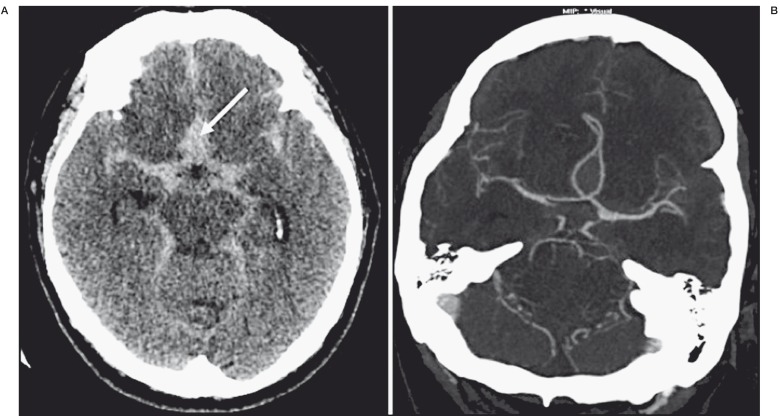
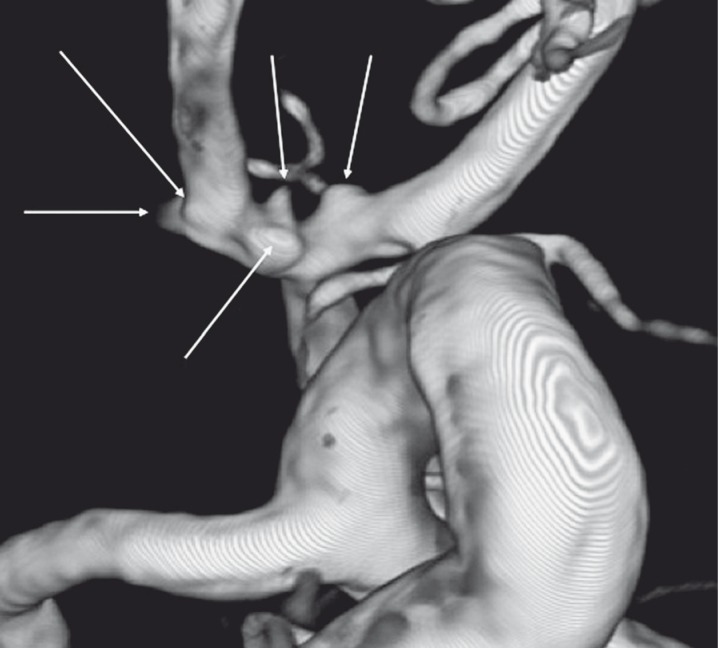
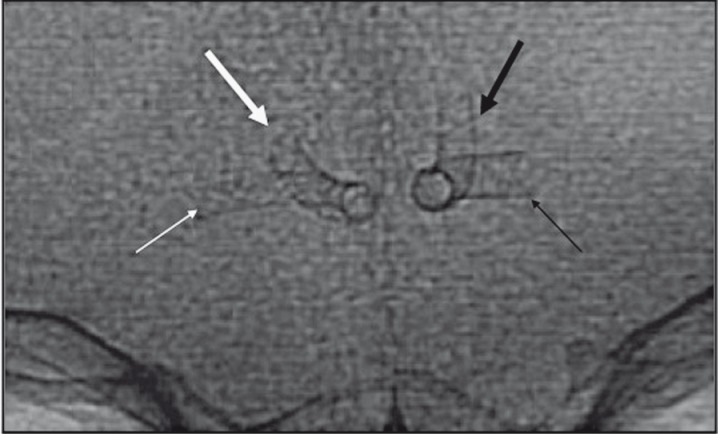
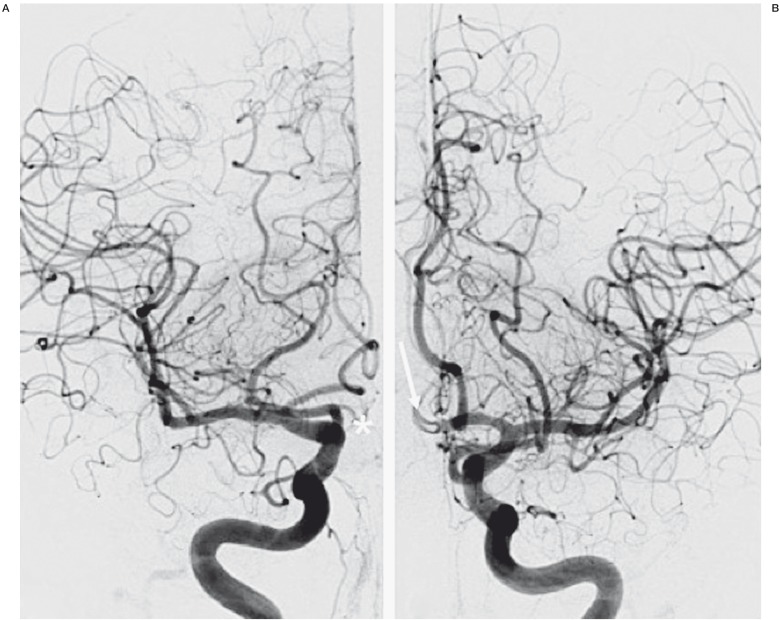
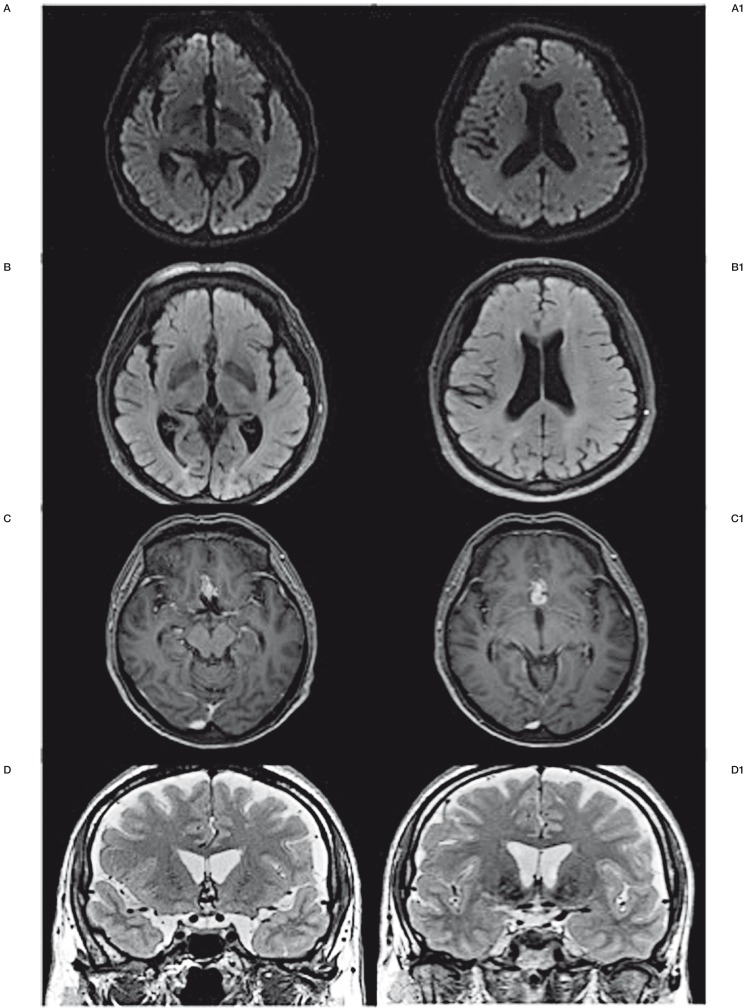
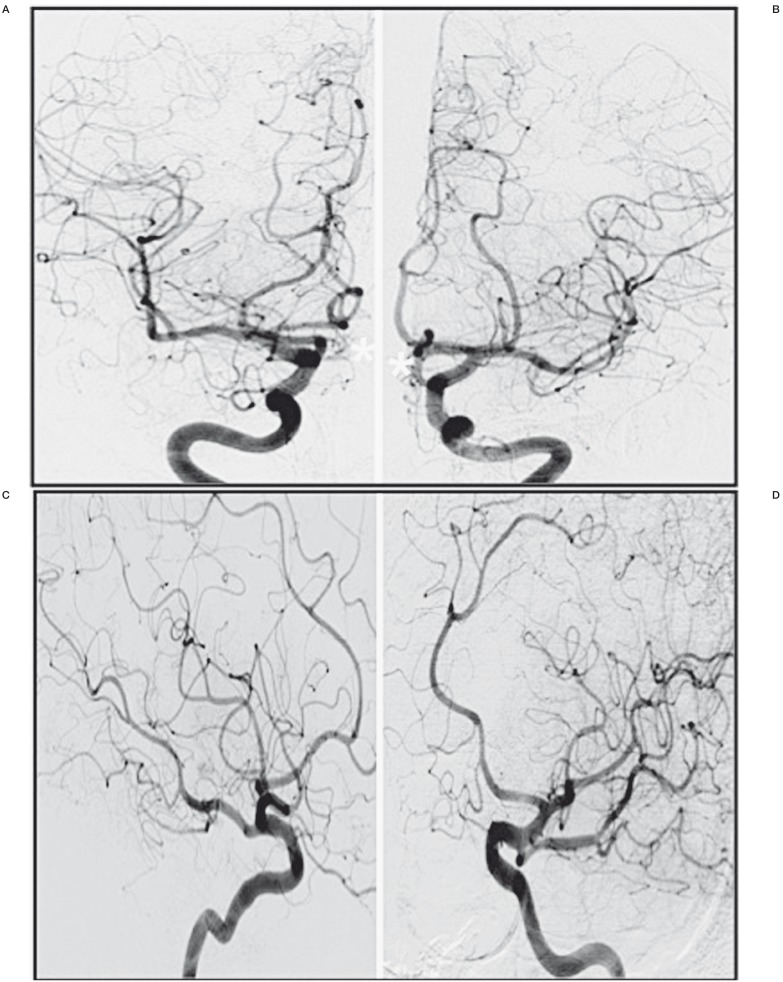
Blood blister-like aneurysms (BLAs) are rare lesions, associated with diffuse subarachnoid hemorrhage (SAH). BLAs tend to rebleed quickly after first bleeding and must be treated as an emergency. Acute treatment is challenging using surgical and endovascular approaches due to the fragile aneurysm wall and small sac. Flow-diverter stents (FDSs) may offer a new option for the treatment of difficult small aneurysms. We describe a case of a ruptured BLA on the anterior communicating artery (AComA) treated in the acute phase of SAH by endovascular exclusion of the AComA with deployment of two FDSs in the A1/A2 junctions of both anterior cerebral arteries (ACAs). A 61-year-old man was admitted for diffuse SAH with a focal interhemispheric hematoma. Angiography revealed multiple arterial wall irregularities on the AComA and both ACAs. We performed an endovascular shunt of the AComA by deploying two FDSs in both A1/A2 junctions. Immediate control injections confirmed flow diversion in the A1/A2 segments of the ACAs with decreased blood flow in the AComA. The patient's course in hospital was uneventful. A three-month follow-up angiogram confirmed complete exclusion of the aneurysms, complete exclusion of the AComA, and patency of the two ACAs without any persistent arterial wall irregularity. Endovascular bypass using an FDS for a ruptured BLA has never been described. It establishes a new therapeutic option despite the need for antiplatelet therapy. Endovascular AComA exclusion using an FDS may be a solution when no other treatment is available for a ruptured BLA.
Keywords: blister-like aneurysm; flow-diverter stent; subarachnoid hemorrhage.
Figures
References
-
- Ezaki Y, Takahata H, Kamada K, et al. Aneurysmal embolization of a blisterlike aneurysm of the internal carotid artery: a case report and review of the literature. Surg Neurol. 2006;65(6):628–630. discussion 630. - PubMed
-
- Park JH, Park IS, Han DH, et al. Endovascular treatment of blood blister-like aneurysms of the internal carotid artery. J Neurosurg. 2007;106(5):812–819. - PubMed
-
- Meling TR, Sorteberg A, Bakke SJ, et al. Blood blister-like aneurysms of the internal carotid artery trunk causing subarachnoid hemorrhage: treatment and outcome. J Neurosurg. 2008;108(4):662–671. - PubMed
-
- Lee BH, Kim BM, Park MS, et al. Reconstructive endovascular treatment of ruptured blood blister-like aneurysms of the internal carotid artery. J Neurosurg. 2009;11(3):431–436. - PubMed
-
- Lee JW, Choi HG, Jung JY, et al. Surgical strategies for ruptured blister-like aneurysms arising from the internal carotid artery: a clinical analysis of 18 consecutive patients. Acta Neurochir (Wien) 2009;151(2):125–130. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
