

Acute microcirculatory effects of medium frequency versus high frequency neuromuscular electrical stimulation in critically ill patients - a pilot study
- PMID: 24355422
- PMCID: PMC3878255
- DOI: 10.1186/2110-5820-3-39
Acute microcirculatory effects of medium frequency versus high frequency neuromuscular electrical stimulation in critically ill patients - a pilot study
Abstract
Background: Intensive care unit-acquired weakness (ICUAW) is a common complication, associated with significant morbidity. Neuromuscular electrical stimulation (NMES) has shown promise for prevention. NMES acutely affects skeletal muscle microcirculation; such effects could mediate the favorable outcomes. However, optimal current characteristics have not been defined. This study aimed to compare the effects on muscle microcirculation of a single NMES session using medium and high frequency currents.
Methods: ICU patients with systemic inflammatory response syndrome (SIRS) or sepsis of three to five days duration and patients with ICUAW were studied. A single 30-minute NMES session was applied to the lower limbs bilaterally using current of increasing intensity. Patients were randomly assigned to either the HF (75 Hz, pulse 400 μs, cycle 5 seconds on - 21 seconds off) or the MF (45 Hz, pulse 400 μs, cycle 5 seconds on - 12 seconds off) protocol. Peripheral microcirculation was monitored at the thenar eminence using near-infrared spectroscopy (NIRS) to obtain tissue O2 saturation (StO2); a vascular occlusion test was applied before and after the session. Local microcirculation of the vastus lateralis was also monitored using NIRS.
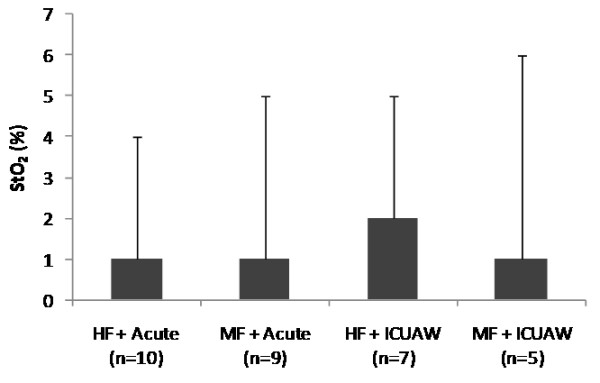
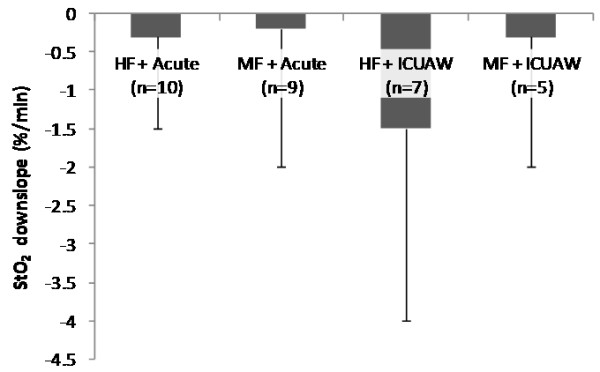
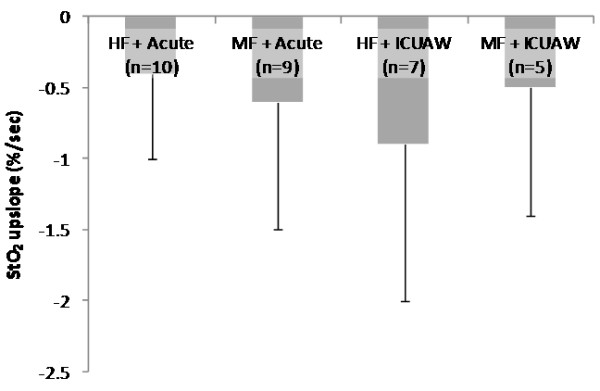
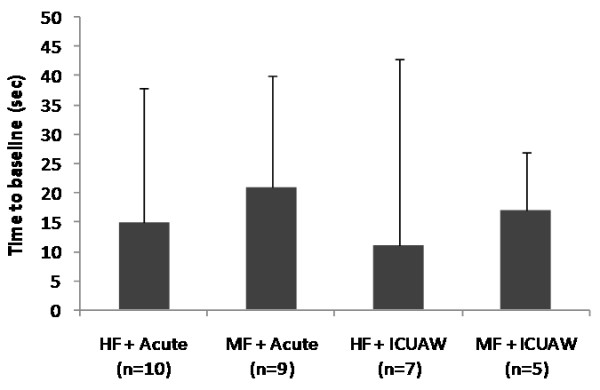
Results: Thirty-one patients were randomized. In the HF protocol (17 patients), peripheral microcirculatory parameters were: thenar O2 consumption rate (%/minute) from 8.6 ± 2.2 to 9.9 ± 5.1 (P = 0.08), endothelial reactivity (%/second) from 2.7 ± 1.4 to 3.2 ± 1.9 (P = 0.04), vascular reserve (seconds) from 160 ± 55 to 145 ± 49 (P = 0.03). In the MF protocol: thenar O2 consumption rate (%/minute) from 8.8 ± 3.8 to 9.9 ± 3.6 (P = 0.07), endothelial reactivity (%/second) from 2.5 ± 1.4 to 3.1 ± 1.7 (P = 0.03), vascular reserve (seconds) from 163 ± 37 to 144 ± 33 (P = 0.001). Both protocols showed a similar effect. In the vastus lateralis, average muscle O2 consumption rate was 61 ± 9%/minute during the HF protocol versus 69 ± 23%/minute during the MF protocol (P = 0.5). The minimum amplitude in StO2 was 5 ± 4 units with the HF protocol versus 7 ± 4 units with the MF protocol (P = 0.3). Post-exercise, StO2 increased by 6 ± 7 units with the HF protocol versus 5 ± 4 units with the MF protocol (P = 0.6). These changes correlated well with contraction strength.
Conclusions: A single NMES session affected local and systemic skeletal muscle microcirculation. Medium and high frequency currents were equally effective.
Figures
References
-
- Garnacho-Montero J, Amaya-Villar R, García-Garmendía JL, Madrazo-Osuna J, Ortiz-Leyba C. Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients. Crit Care Med. 2005;3:349–354. doi: 10.1097/01.CCM.0000153521.41848.7E. - DOI - PubMed
-
- Zifko UA. Long-term outcome of critical illness polyneuropathy. Muscle Nerve Suppl. 2000;3:S49–S52. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
