

Relevant issues in the pathology and pathobiology of pulmonary hypertension
- PMID: 24355640
- PMCID: PMC3970402
- DOI: 10.1016/j.jacc.2013.10.025
Relevant issues in the pathology and pathobiology of pulmonary hypertension
Abstract
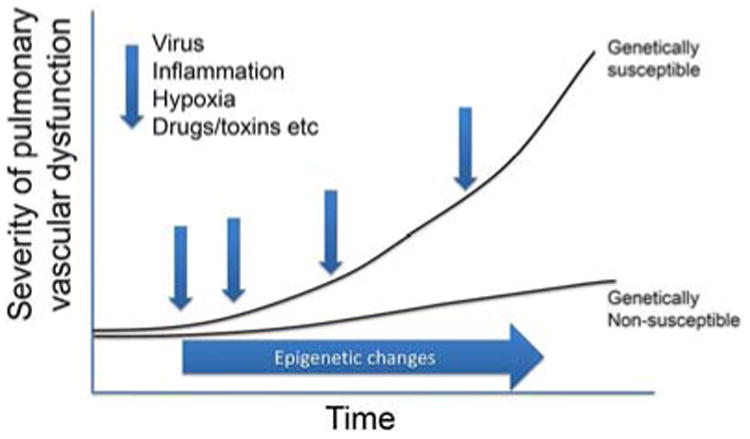
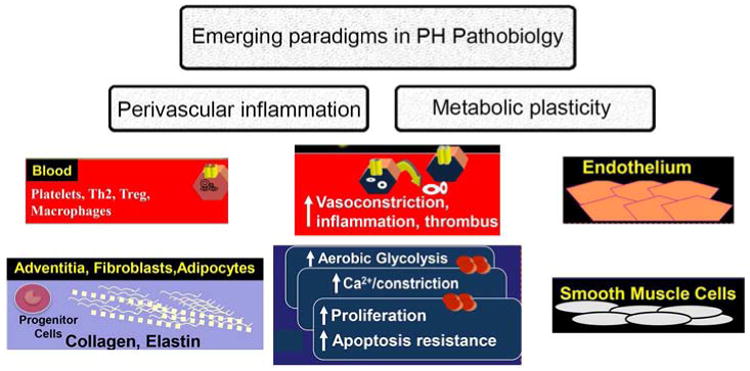
Knowledge of the pathobiology of pulmonary hypertension (PH) continues to accelerate. However, fundamental gaps remain in our understanding of the underlying pathological changes in pulmonary arteries and veins in the different forms of this syndrome. Although PH primarily affects the arteries, venous disease is increasingly recognized as an important entity. Moreover, prognosis in PH is determined largely by the status of the right ventricle, rather than the levels of pulmonary artery pressures. It is increasingly clear that although vasospasm plays a role, PH is an obstructive lung panvasculopathy. Disordered metabolism and mitochondrial structure, inflammation, and dysregulation of growth factors lead to a proliferative, apoptosis-resistant state. These abnormalities may be acquired, genetically mediated as a result of mutations in bone morphogenetic protein receptor-2 or activin-like kinase-1, or epigenetically inherited (as a result of epigenetic silencing of genes such as superoxide dismutase-2). There is a pressing need to better understand how the pathobiology leads to severe disease in some patients versus mild PH in others. Recent recognition of a potential role of acquired abnormalities of mitochondrial metabolism in the right ventricular myocytes and pulmonary vascular cells suggests new therapeutic approaches, diagnostic modalities, and biomarkers. Finally, dissection of the role of pulmonary inflammation in the initiation and promotion of PH has revealed a complex yet fascinating interplay with pulmonary vascular remodeling, promising to lead to novel therapeutics and diagnostics. Emerging concepts are also relevant to the pathobiology of PH, including a role for bone marrow and circulating progenitor cells and microribonucleic acids. Continued interest in the interface of the genetic basis of PH and cellular and molecular pathogenetic links should further expand our understanding of the disease.
Keywords: ALK; BMPR2; DC; ER; HIF; IPAH; LHF; PAH; PH; activin receptor-like kinase; bone morphogenetic protein type II receptor; dendritic cell; endoplasmic reticulum; hypoxia inducible factor; idiopathic pulmonary arterial hypertension; inflammation; left heart failure; metabolism; pulmonary arterial hypertension; pulmonary arteries; pulmonary hypertension; pulmonary veins.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
SLA has no conflict of interest to declare
PD declares what follows: Speaker fees for meetings supported by Actelion Pharmaceuticals, France.
SCE has no conflict of interest to declare
CG has no conflict of interest to declare
EM declares what follows: Medtelligence Steering Committee (young invesitgators selection committee); Bayer (clinical trial Steering Committee); Both < USD 10.000,00 total in the past 2 years
MR has no conflict of interest to declare
RTS declares what follows: Unrestricred research grants from Actelion, Bayer-Healthcare, Novartis, Noxxon, Pfizer
KRS has no conflict of interest to declare
NM has no conflict of interest to declare
Figures
Republished in
-
[Relevant issues in the pathology and pathobiology of pulmonary hypertension].Turk Kardiyol Dern Ars. 2014 Oct;42 Suppl 1:5-16. Turk Kardiyol Dern Ars. 2014. PMID: 25697030 Turkish.
References
-
- Tuder RM, Abman SH, Braun T, et al. Development and pathology of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S3–S9. - PubMed
-
- Merklinger SL, Jones PL, Martinez EC, Rabinovitch M. Epidermal growth factor receptor blockade mediates smooth muscle cell apoptosis and improves survival in rats with pulmonary hypertension. Circulation. 2005;112:423–31. - PubMed
Publication types
MeSH terms
Grants and funding
- RC1 HL 10084/HL/NHLBI NIH HHS/United States
- R37 HL060917/HL/NHLBI NIH HHS/United States
- 1R01HL114887/HL/NHLBI NIH HHS/United States
- F32 HL010084/HL/NHLBI NIH HHS/United States
- NIH-RO1-HL071115/HL/NHLBI NIH HHS/United States
- R01 HL060917/HL/NHLBI NIH HHS/United States
- NIH/NHLBI SCCOR 5P50HL084923/PHS HHS/United States
- RG/13/4/30107/BHF_/British Heart Foundation/United Kingdom
- HL60917/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- P01 HL108797/HL/NHLBI NIH HHS/United States
- R01 HL071115/HL/NHLBI NIH HHS/United States
- P50 HL084923/HL/NHLBI NIH HHS/United States
- R01 HL115008/HL/NHLBI NIH HHS/United States
- R01 HL113003/HL/NHLBI NIH HHS/United States
- P01 HL014985/HL/NHLBI NIH HHS/United States
- 1RC1HL099462/HL/NHLBI NIH HHS/United States
- HL115008/HL/NHLBI NIH HHS/United States
- R01 HL114887/HL/NHLBI NIH HHS/United States
- NIH PPG 5P01HL014985/HL/NHLBI NIH HHS/United States
- RC1 HL100849/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
