

Follow-up of true visceral artery aneurysm after coil embolization by three-dimensional contrast-enhanced MR angiography
- PMID: 24356294
- PMCID: PMC4463299
- DOI: 10.5152/dir.2013.13236
Follow-up of true visceral artery aneurysm after coil embolization by three-dimensional contrast-enhanced MR angiography
Abstract
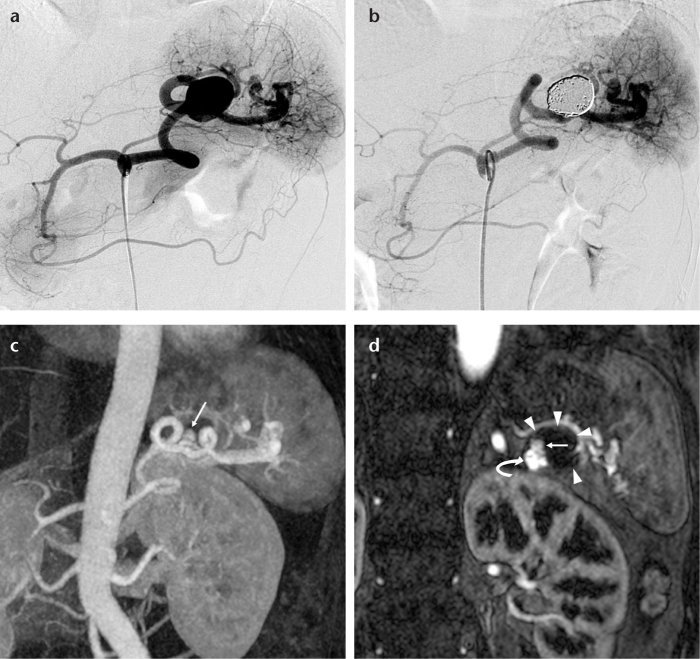
Purpose: We aimed to evaluate the outcomes of coil embolization of true visceral artery aneurysms by three-dimensional contrast-enhanced magnetic resonance (MR) angiography.
Materials and methods: We used three-dimensional contrast-enhanced MR angiography, which included source images, to evaluate 23 patients (mean age, 60 years; range, 28-83 years) with true visceral artery aneurysms (splenic, n=15; hepatic, n=2; gastroduodenal, n=2; celiac, n=2; pancreaticoduodenal, n=1; gastroepiploic, n=1) who underwent coil embolization. Angiographic aneurysmal occlusion was revealed in all cases. Follow-up MR angiography was conducted with either a 1.5 or 3 Tesla system 3-25 months (mean, 18 months) after embolization. MR angiography was evaluated for aneurysmal occlusion, hemodynamic status, and complications.
Results: Complete aneurysmal occlusion was determined in 22 patients (96%) on follow-up MR angiography (mean follow-up period, 18 months). Neck recanalization, which was observed at nine and 20 months after embolization, was confirmed in one of eight patients (13%) using a neck preservation technique. In this patient, a small neck recanalization covered by a coil mass was demonstrated. The complete hemodynamic status after embolization was determined in 21 patients (91%); the visualization of several collateral vessels, such as short gastric arteries, after parent artery occlusion was poor compared with that seen on digital subtraction angiography in the remaining two patients (9%). An asymptomatic localized splenic infarction was confirmed in one patient (4%).
Conclusion: Our study presents the follow-up results from three-dimensional contrast-enhanced MR angiography, which confirmed neck recanalization, the approximate hemodynamic status, and complications. This effective and less invasive method may be suitable for serial follow-up after coil embolization of true visceral aneurysms.
Figures



References
-
- Carmeci C, McClenathan J. Visceral artery aneurysms as seen in a community hospital. Am J Surg. 2000;179:486–489. - PubMed
-
- Kalko Y, Ugurlucan M, Basaran M, et al. Visceral artery aneurysms. Heart Surg Forum. 2007;10:E24–29. - PubMed
-
- Shanley CJ, Shah NL, Messina LM. Common splanchnic artery aneurysms: splenic, hepatic, and celiac. Ann Vasc Surg. 1996;10:315–322. - PubMed
-
- Wagner WH, Allins AD, Treiman RL, et al. Ruptured visceral artery aneurysms. Ann Vasc Surg. 1997;11:342–347. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
