

Right ventricular dysfunction in chronic thromboembolic obstruction of the pulmonary artery: a pressure-volume study using the conductance catheter
- PMID: 24356516
- PMCID: PMC3921352
- DOI: 10.1152/japplphysiol.01123.2013
Right ventricular dysfunction in chronic thromboembolic obstruction of the pulmonary artery: a pressure-volume study using the conductance catheter
Abstract
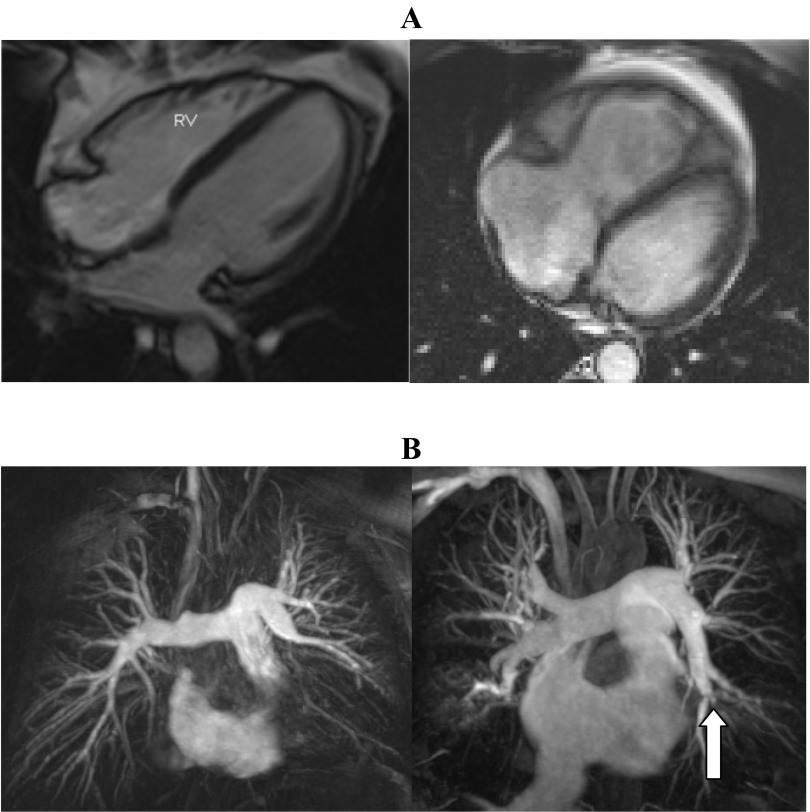
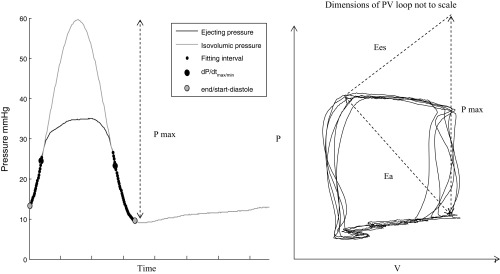
Pressure-volume loops describe dynamic ventricular performance, relevant to patients with and at risk of pulmonary hypertension. We used conductance catheter-derived pressure-volume loops to measure right ventricular (RV) mechanics in patients with chronic thromboembolic pulmonary arterial obstruction at different stages of pathological adaptation. Resting conductance catheterization was performed in 24 patients: 10 with chronic thromboembolic pulmonary hypertension (CTEPH), 7 with chronic thromboembolic disease without pulmonary hypertension (CTED), and 7 controls. To assess the validity of conductance measurements, RV volumes were compared in a subset of 8 patients with contemporaneous cardiac magnetic resonance (CMR). Control, CTED, and CTEPH groups showed different pressure-volume loop morphology, most notable during systolic ejection. Prolonged diastolic relaxation was seen in patients with CTED and CTEPH [tau = 56.2 ± 6.7 (controls) vs. 69.7 ± 10.0 (CTED) vs. 67.9 ± 6.2 ms (CTEPH), P = 0.02]. Control and CTED groups had lower afterload (Ea) and contractility (Ees) compared with the CTEPH group (Ea = 0.30 ± 0.10 vs. 0.52 ± 0.24 vs. 1.92 ± 0.70 mmHg/ml, respectively, P < 0.001) (Ees = 0.44 ± 0.20 vs. 0.59 ± 0.15 vs. 1.13 ± 0.43 mmHg/ml, P < 0.01) with more efficient ventriculoarterial coupling (Ees/Ea = 1.46 ± 0.30 vs. 1.27 ± 0.36 vs. 0.60 ± 0.18, respectively, P < 0.001). Stroke volume assessed by CMR and conductance showed closest agreement (mean bias +9 ml, 95% CI -1 to +19 ml) compared with end-diastolic volume (+48 ml, -16 to 111 ml) and end-systolic volume (+37 ml, -21 to 94 ml). RV conductance catheterization detects novel alteration in pressure-volume loop morphology and delayed RV relaxation in CTED, which distinguish this group from controls. The observed agreement in stroke volume assessed by CMR and conductance suggests RV mechanics are usefully measured by conductance catheter in chronic thromboembolic obstruction.
Keywords: chronic thromboembolism; diastolic dysfunction; pulmonary hypertension; right ventricle.
Figures



References
-
- Baan J, Jong TT, Kerkhof PL, Moene RJ, van Dijk AD, van der Velde ET, Koops J. Continuous stroke volume and cardiac output from intra-ventricular dimensions obtained with impedance catheter. Cardiovasc Res 15: 328–334, 1981 - PubMed
-
- Baan J, van der Velde ET, de Bruin HG, Smeenk GJ, Koops J, van Dijk AD, Temmerman D, Senden J, Buis B. Continuous measurement of left ventricular volume in animals and humans by conductance catheter. Circulation 70: 812–823, 1984 - PubMed
-
- Bishop A, White P, Chaturvedi R, Brookes C, Redington A, Oldershaw P. Resting right ventricular function in patients with coronary artery disease: pressure volume analysis using conductance catheters. Int J Cardiol 58: 223–228, 1997 - PubMed
-
- Bonderman D, Martischnig AM, Vonbank K, Nikfardjam M, Meyer B, Heinz G, Klepetko W, Naeije R, Lang IM. Right ventricular load at exercise is a cause of persistent exercise limitation in patients with normal resting pulmonary vascular resistance after pulmonary endarterectomy. Chest 139: 122–127, 2011 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical