

Enhanced recovery after bariatric surgery (ERABS): clinical outcomes from a tertiary referral bariatric centre
- PMID: 24357126
- PMCID: PMC3972428
- DOI: 10.1007/s11695-013-1151-4
Enhanced recovery after bariatric surgery (ERABS): clinical outcomes from a tertiary referral bariatric centre
Abstract
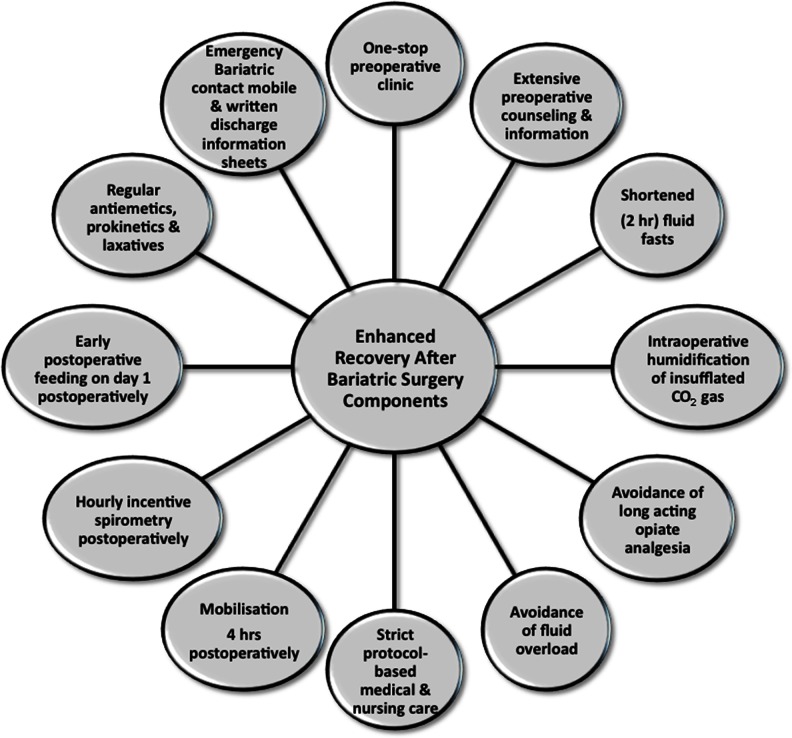
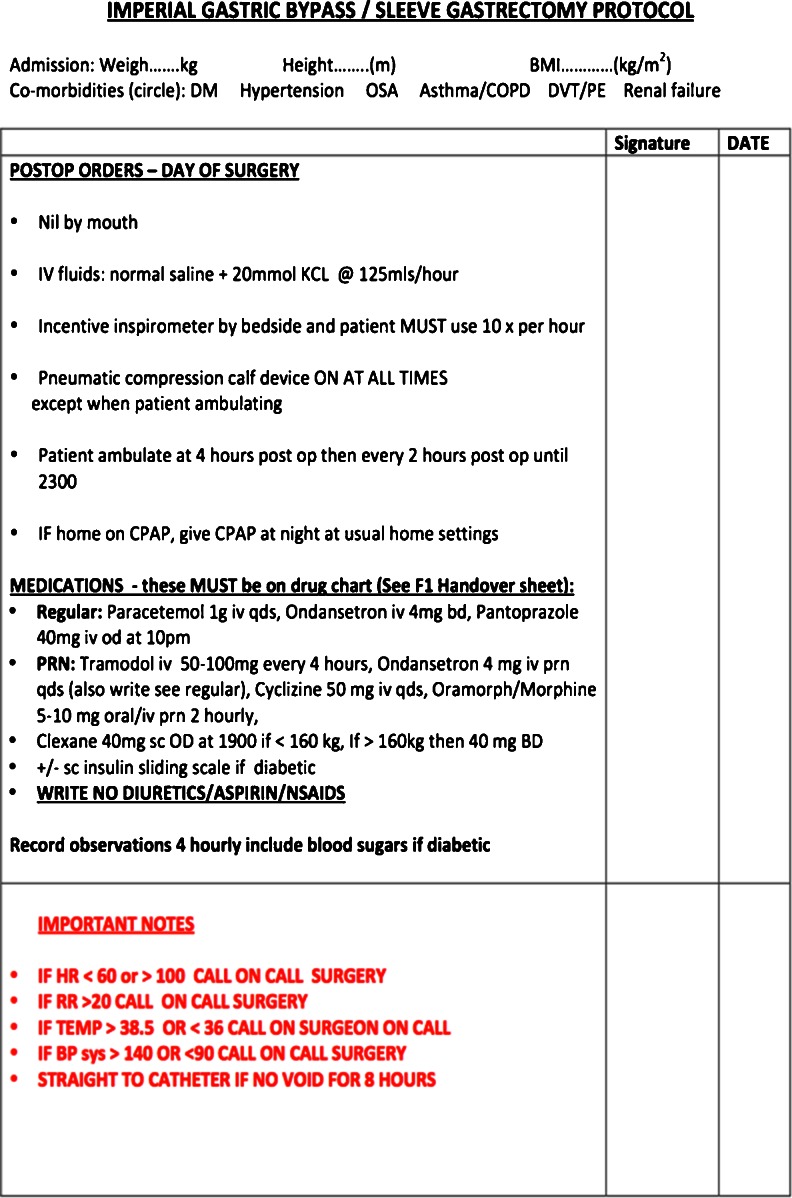
There is paucity of data on Enhanced Recovery After Bariatric Surgery (ERABS) protocols. This feasibility study reports outcomes of this protocol utilized within a tertiary-referral bariatric centre. Data on consecutive primary procedures (laparoscopic gastric bypasses, sleeve gastrectomies and gastric bands) performed over 9 months within an ERABS protocol were prospectively recorded. Interventions utilized included shortened preoperative fasts, intra-operative humidification, early mobilization and feeding, avoidance of fluid overload, incentive spirometry, use of prokinetics and laxatives. Data collected included demographics, co-morbidities, morbidity, mortality, length of stay (LOS) and re-admissions. A total of 226 procedures (age [mean ± SD], 45 ± 11 years, median [interquartile range] BMI 44.9 [41.0-49.0] kg/m2) were undertaken: 150 (66%) bypasses, 47 (21%) sleeves and 29 (13%) bands. Hypertension, diabetes mellitus, sleep apnea and limited mobility were present in 40%, 34%, 24% and 9% of patients, respectively. No anastomotic or staple line leaks/bleeds were encountered. Ten (4.4%) patients developed postoperative morbidity (mainly respiratory complications). One death occurred from massive pulmonary embolus in a high-risk patient (despite insertion of preoperative-IVC filter). Respective mean ± SD LOS for bypasses, sleeves and bands were 1.88 ± 1.12, 2.30 ± 1.69 and 0.69 ± 0.81 days. Successful discharge on the first postoperative day was achieved in 37% and 28% of bypasses and sleeves, respectively. Day-case gastric bands were performed in 48%. Thirty-day hospital re-admission occurred in six (2.7%) patients. Applying an ERABS protocol was feasible, safe, associated with low morbidity, acceptable LOS and low 30-day re-admission rates. The presence of multiple medical co-morbidities should not preclude use of an ERABS protocol within bariatric patients.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
