

Cost-effectiveness of prenatal screening strategies for congenital heart disease
- PMID: 24357432
- PMCID: PMC5278773
- DOI: 10.1002/uog.13287
Cost-effectiveness of prenatal screening strategies for congenital heart disease
Abstract
Objective: The economic implications of strategies to improve prenatal screening for congenital heart disease (CHD) in low-risk mothers have not been explored. The aim was to perform a cost-effectiveness analysis of different screening methods.
Methods: We constructed a decision analytic model of CHD prenatal screening strategies (four-chamber screen (4C), 4C + outflow, nuchal translucency (NT) or fetal echocardiography) populated with probabilities from the literature. The model included whether initial screens were interpreted by a maternal-fetal medicine (MFM) specialist and different referral strategies if they were read by a non-MFM specialist. The primary outcome was the incremental cost per defect detected. Costs were obtained from Medicare National Fee estimates. A probabilistic sensitivity analysis was undertaken on model variables commensurate with their degree of uncertainty.
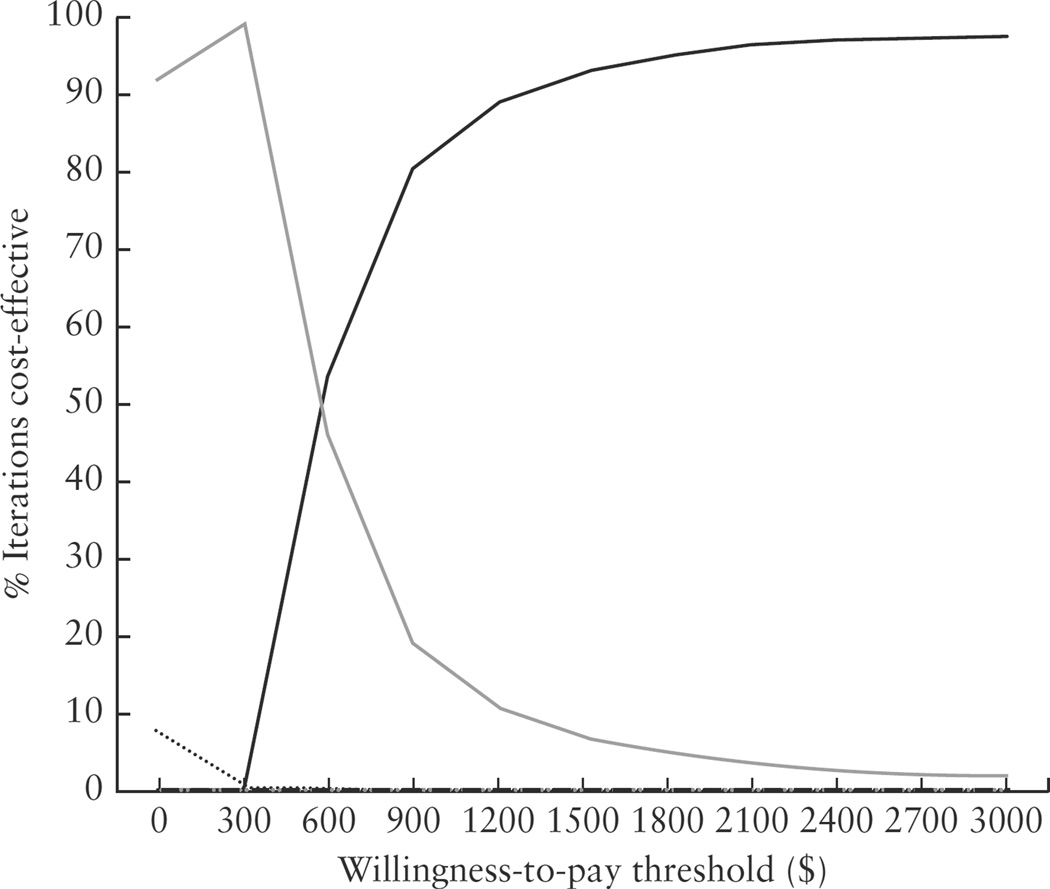
Results: In base-case analysis, 4C + outflow referred to an MFM specialist was the least costly strategy per defect detected. The 4C screen and the NT screen were dominated by other strategies (i.e. were more costly and less effective). Fetal echocardiography was the most effective, but most costly. On simulation of 10 000 low-risk pregnancies, 4C + outflow screen referred to an MFM specialist remained the least costly per defect detected. For an additional $580 per defect detected, referral to cardiology after a 4C + outflow was the most cost-effective for the majority of iterations, increasing CHD detection by 13 percentage points.
Conclusions: The addition of examination of the outflow tracts to second-trimester ultrasound increases detection of CHD in the most cost-effective manner. Strategies to improve outflow-tract imaging and to refer with the most efficiency may be the best way to improve detection at a population level.
Keywords: congenital heart disease; cost; cost analysis; nuchal translucency measurement; prenatal diagnosis; prenatal ultrasound.
Copyright © 2013 ISUOG. Published by John Wiley & Sons Ltd.
Figures
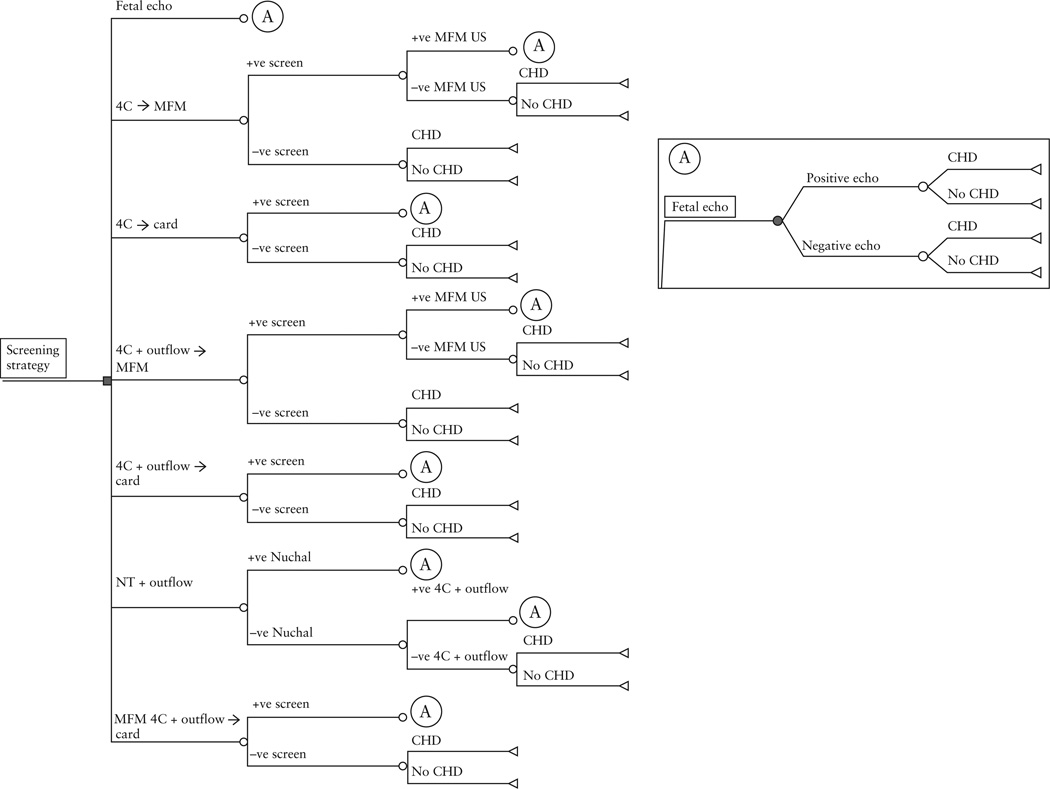
 , 4C→card, standard screen with second-trimester ultrasound of the four-chamber view of the heart, with referral to a pediatric cardiologist if abnormal;
, 4C→card, standard screen with second-trimester ultrasound of the four-chamber view of the heart, with referral to a pediatric cardiologist if abnormal;  , 4C + outflow → MFM, screen with second-trimester ultrasound four-chamber and outflow views of the heart (read by a non-MFM specialist), with referral to an MFM specialist if abnormal;
, 4C + outflow → MFM, screen with second-trimester ultrasound four-chamber and outflow views of the heart (read by a non-MFM specialist), with referral to an MFM specialist if abnormal;  , 4C + outflow → card, screen with second-trimester ultrasound four-chamber and outflow views of the heart (read by a non-MFM specialist), with referral to a pediatric cardiologist if abnormal;
, 4C + outflow → card, screen with second-trimester ultrasound four-chamber and outflow views of the heart (read by a non-MFM specialist), with referral to a pediatric cardiologist if abnormal;  , MFM 4C + outflow → card, screen with second-trimester ultrasound four-chamber and outflow views of the heart, interpreted by an MFM specialist and referred to a pediatric cardiologist if abnormal;
, MFM 4C + outflow → card, screen with second-trimester ultrasound four-chamber and outflow views of the heart, interpreted by an MFM specialist and referred to a pediatric cardiologist if abnormal;  , NT + outflow, tiered screen with first-trimester nuchal translucency and referral directly for fetal echocardiography if abnormal; if normal, screen with second-trimester ultrasound four chamber and outflow views.
, NT + outflow, tiered screen with first-trimester nuchal translucency and referral directly for fetal echocardiography if abnormal; if normal, screen with second-trimester ultrasound four chamber and outflow views.  , Fetal echo, universal screen with fetal echocardiography.
, Fetal echo, universal screen with fetal echocardiography.References
-
- Hoffman JI. Incidence of congenital heart disease: II. Prenatal incidence. Pediatr Cardiol. 1995;16:155–165. - PubMed
-
- Kleinert S. Routine prenatal screening for congenital heart disease. Lancet. 1996;348:836. - PubMed
-
- Stumpfen I, Stumpfen A, Wimmer M, Bernaschek G. Effect of detailed fetal echocardiography as part of routine prenatal ultrasonographic screening on detection of congenital heart disease. Lancet. 1996;348:854–857. - PubMed
-
- AIUM Practice Guideline for the Performance of Obstetric Ultrasound Examinations. J Ultrasound Med. 2013;32:1083–1101. - PubMed
-
- AIUM Practice Guideline for the Performance of Obstetric Ultrasound Examinations. J Ultrasound Med. 2010;29:157–166. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
