

Autoinflammatory bone disorders with special focus on chronic recurrent multifocal osteomyelitis (CRMO)
- PMID: 24359092
- PMCID: PMC3881012
- DOI: 10.1186/1546-0096-11-47
Autoinflammatory bone disorders with special focus on chronic recurrent multifocal osteomyelitis (CRMO)
Abstract
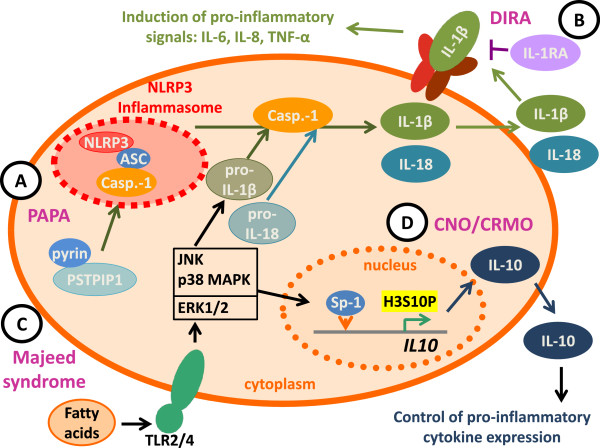
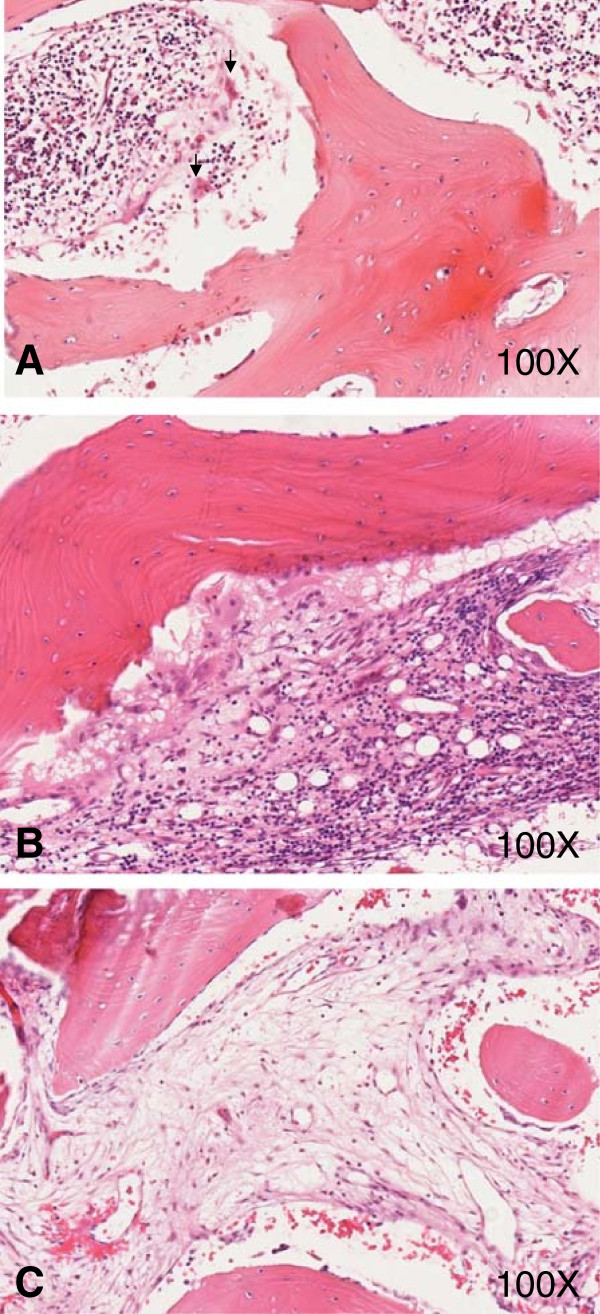
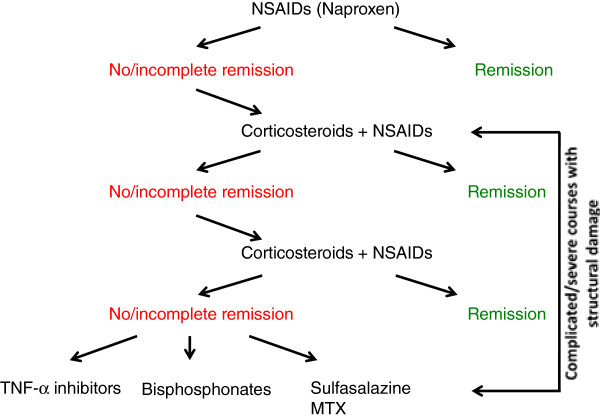
Sterile bone inflammation is the hallmark of autoinflammatory bone disorders, including chronic nonbacterial osteomyelitis (CNO) with its most severe form chronic recurrent multifocal osteomyelitis (CRMO). Autoinflammatory osteopathies are the result of a dysregulated innate immune system, resulting in immune cell infiltration of the bone and subsequent osteoclast differentiation and activation. Interestingly, autoinflammatory bone disorders are associated with inflammation of the skin and/or the intestine. In several monogenic autoinflammatory bone disorders mutations in disease-causing genes have been reported. However, regardless of recent developments, the molecular pathogenesis of CNO/CRMO remains unclear.Here, we discuss the clinical presentation and molecular pathophysiology of human autoinflammatory osteopathies and animal models with special focus on CNO/CRMO. Treatment options in monogenic autoinflammatory bone disorders and CRMO will be illustrated.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
