

Height and risk of sudden cardiac death: the Atherosclerosis Risk in Communities and Cardiovascular Health studies
- PMID: 24360853
- PMCID: PMC3945001
- DOI: 10.1016/j.annepidem.2013.11.008
Height and risk of sudden cardiac death: the Atherosclerosis Risk in Communities and Cardiovascular Health studies
Abstract
Purpose: Sudden cardiac death (SCD) is an important cause of mortality in the adult population. Height has been associated with cardiac hypertrophy and an increased risk of arrhythmias but also with decreased risk of coronary heart disease, suggesting a complex association with SCD.
Methods: We examined the association of adult height with the risk of physician-adjudicated SCD in two large population-based cohorts: the Cardiovascular Health Study and the Atherosclerosis Risk in Communities study.
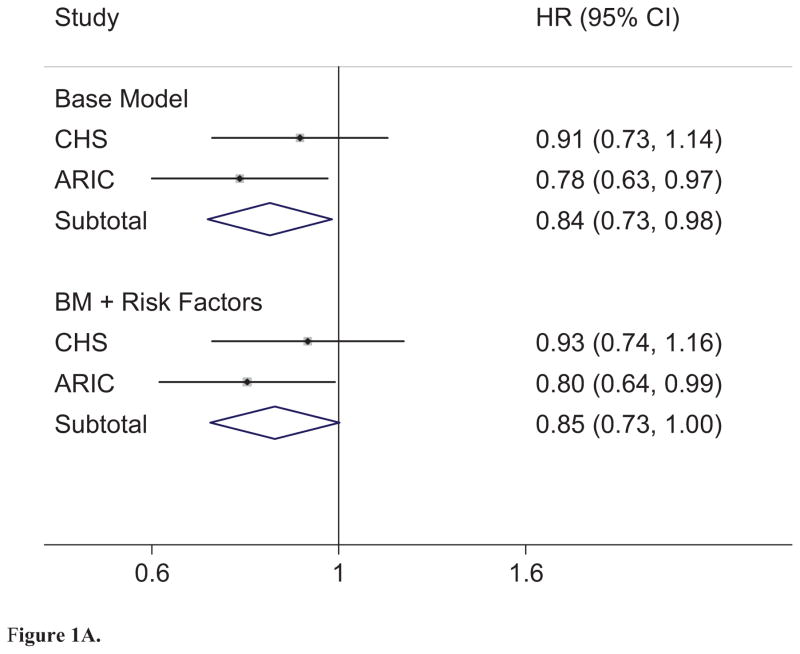
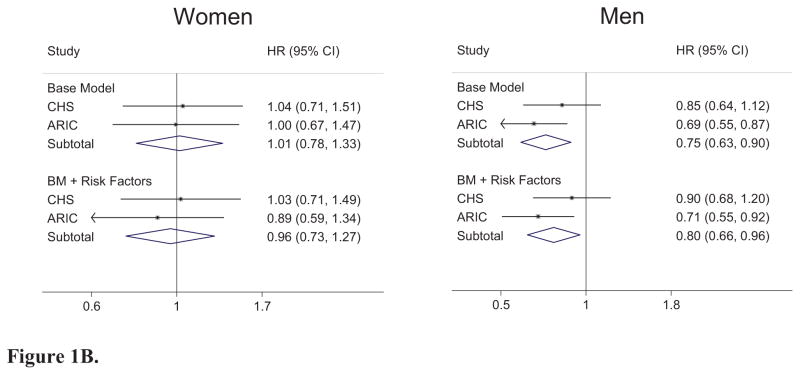
Results: Over an average follow-up time of 11.7 years in Cardiovascular Health Study, there were 199 (3.6%) cases of SCD among 5556 participants. In Atherosclerosis Risk in Communities study, over 12.6 years, there were 227 (1.5%) cases of SCD among 15,633 participants. In both cohorts, there was a trend toward decreased SCD with taller height. In fixed effects meta-analysis, the pooled hazard ratio per 10 cm of height was 0.84; 95% confidence interval, 0.73-0.98; P = .03. The association of increased height with lower risk of SCD was slightly attenuated after inclusion of risk factors associated with height, such as hypertension and left ventricular hypertrophy. The association appeared stronger among men than women in both cohorts.
Conclusions: In two population-based prospective cohorts of different ages, greater height was associated with lower risk of SCD.
Keywords: Body height; Cardiac; Death; Risk factors; Sudden.
Published by Elsevier Inc.
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010 Feb 23;121(7):e46–e215. Epub 2009/12/19.eng. - PubMed
-
- Haider AW, Larson MG, Benjamin EJ, Levy D. Increased left ventricular mass and hypertrophy are associated with increased risk for sudden death. J Am Coll Cardiol. 1998 Nov;32(5):1454–9. Epub 1998/11/11.eng. - PubMed
-
- Verma A, Meris A, Skali H, Ghali JK, Arnold JM, Bourgoun M, et al. Prognostic implications of left ventricular mass and geometry following myocardial infarction: the VALIANT (VALsartan In Acute myocardial iNfarcTion) Echocardiographic Study. JACC Cardiovasc Imaging. 2008 Sep;1(5):582–91. Epub 2009/04/10.eng. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC55222/HC/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- AG023629/AG/NIA NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
