

Single and multiple respiratory virus infections and severity of respiratory disease: a systematic review
- PMID: 24361079
- PMCID: PMC7106320
- DOI: 10.1016/j.prrv.2013.11.001
Single and multiple respiratory virus infections and severity of respiratory disease: a systematic review
Abstract
Introduction: There are suggestions that virus co-infections may influence the clinical outcome of respiratory virus illness. We performed a systematic review of the literature to summarise the evidence.
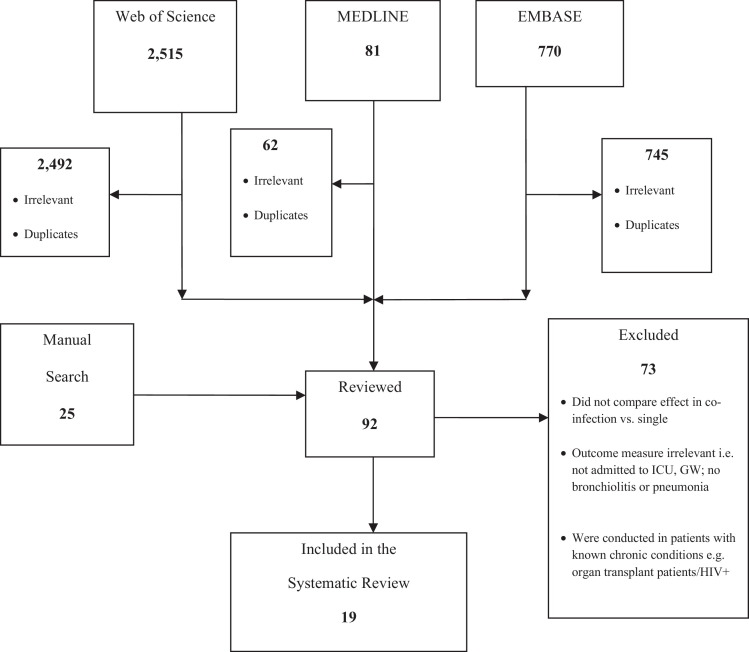
Methods: MEDLINE, EMBASE, Ovid and WEB of Science databases, major organisation websites and reference lists of published studies were searched. The quality of studies was assessed using the STROBE tool (von Elm et al., 1) Individual study data was analyzed using odds ratios and 95% confidence intervals as a measure of association between exposure (co-infection), patient outcome and results summarised using forest plots and tables
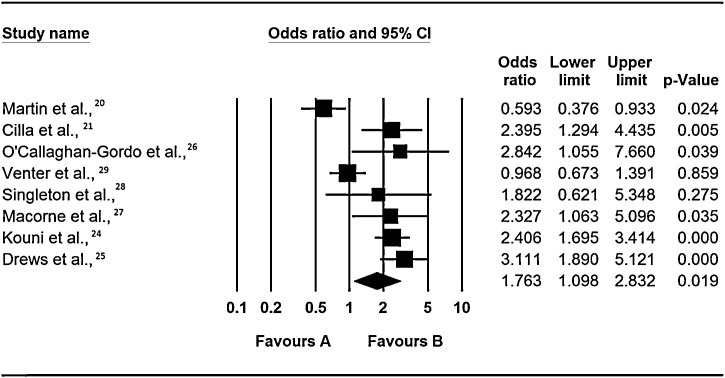
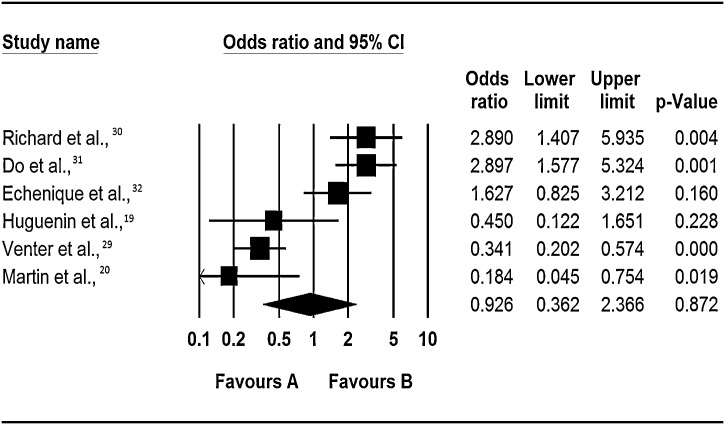
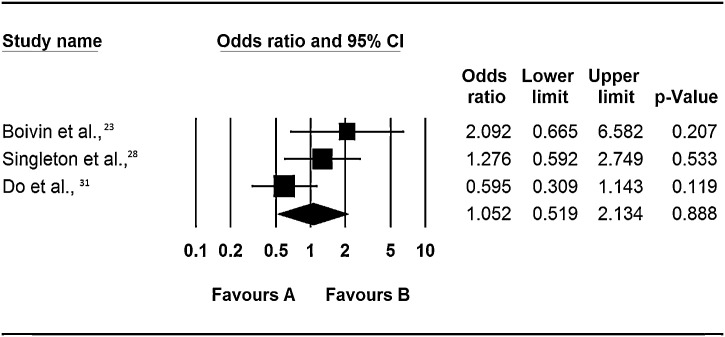
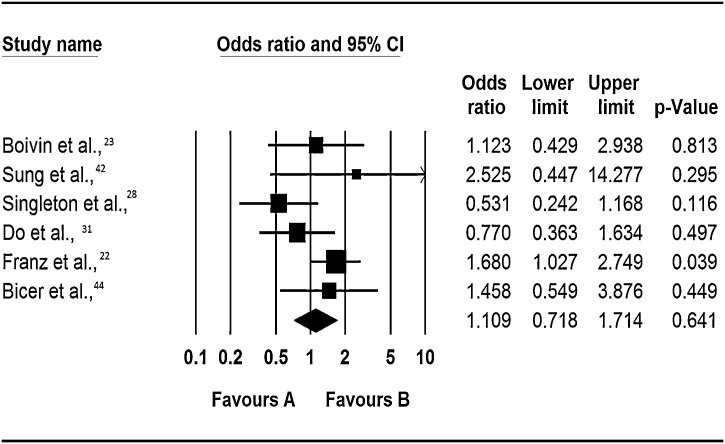
Results: Nineteen (19) studies from all over the world were identified and included in the review. Most of the studies 73.7% (14/19) recruited children ≤ 6 years old. Evidence on the role of co-infection in increasing disease severity was inconclusive. In five out of eight studies, co-infection significantly increased risk of admission to general ward (OR: 2.4, 95% CI: 1.3 - 4.4, p = 0.005; OR: 2.4, 95% CI: 1.1 - 7.7, P = 0.04; OR: 3.1, 95% CI: 2.0 - 5.1, p = <0.001; OR: 2.4, 95% CI: 1.7-3.4, p = <0.0001 and OR: 2.3, 95% CI: 1.1 - 5.1, p = 0.34), one found it did not (OR: 0.59, 95% CI: 0.4 - 0.9, p = 0.02) and the other 2 had insignificant results. Similarly on risk of admission to ICU, some studies found that co-infection significantly increased risk of admission to ICU (OR: 2.9, 95% CI: 1.4 - 5.9, p = 0.004 and OR: 3.0, 95% CI: 1.7 - 5.6, p = <0.0001), whereas others did not (OR: 0.18, 95% CI: 0.05 - 0.75, p = 0.02 and OR: 0.3, 95% CI: 0.2 - 0.6, p = <0.0001). There was no evidence for or against respiratory virus co-infections and risk of bronchiolitis or pneumonia.
Conclusion: The influence of co-infections on severe viral respiratory disease is still unclear. The observed conflict in outcomes could be because they were conducted in different seasons and covered different years and periods. It could also be due to bias towards the null, especially in studies where only crude analysis was conducted. Future studies should employ stratified analysis.
Keywords: admission to ICU; admission to a general ward; co-infections; disease severity; dual or multiple infections; repisratory virus infections.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- von E.E., Altman D.G., Egger M., Pocock S.J., Gotzsche P.C., Vandenbroucke J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. - PubMed
-
- Allander T. Human bocavirus. J Clin Virol. 2008;41(1):29–33. - PubMed
-
- Pyrc K., Berkhout B., van der Hoek L. Identification of new human coronaviruses. Expert Rev Anti Infect Ther. 2007;5(2):245–253. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
