

Variability of resting energy expenditure in infants and young children with intestinal failure-associated liver disease
- PMID: 24361903
- PMCID: PMC5025756
- DOI: 10.1097/MPG.0000000000000288
Variability of resting energy expenditure in infants and young children with intestinal failure-associated liver disease
Abstract
Objective: The aim of the study was to determine, in a cohort of young children with intestinal failure (IF), whether the estimates of basal metabolic rate (BMR) by standard equations can approximate measured resting energy expenditure (REE) by indirect calorimetry (IC).
Methods: IC was performed using the dilutional canopy technique. REE measurements were compared with standard, age-based estimation equations (World Health Organization) for BMR. Subjects were classified as hypermetabolic (REE > 110% BMR), hypometabolic (REE < 90% BMR), or normal (REE = 90%-110% BMR).
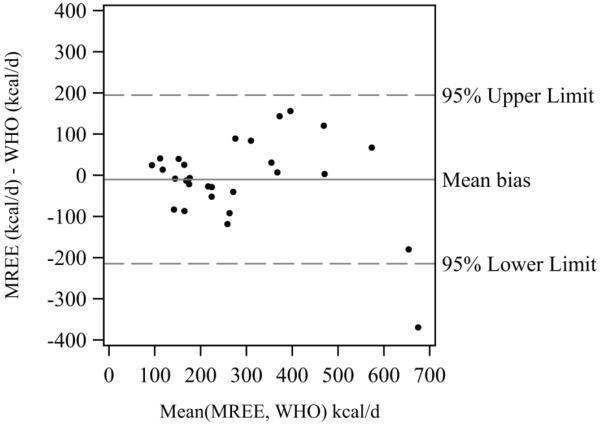
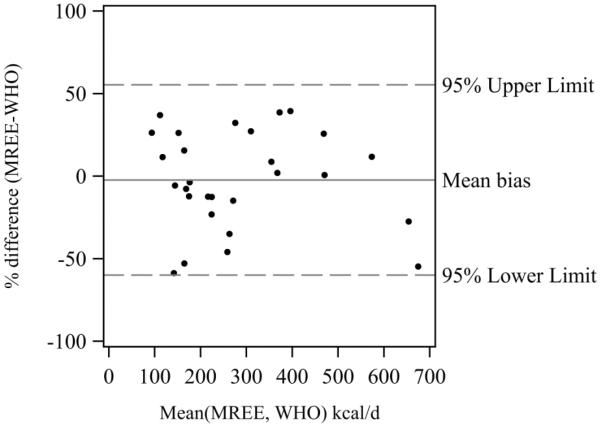
Results: Twenty-eight IF patients (11 girls, 17 boys) had an underlying diagnosis of necrotizing enterocolitis (n = 10) or a congenital gastrointestinal defect (n = 18). Median age was 5.3 months. Median interquartile range (IQR) REE was 46 (42-58) kcal · kg · day. Median (IQR) total energy intake provided 209% (172%-257%) of REE, with parenteral nutrition providing 76% (23%) of total energy intake. REE was variable, with 39% (n = 11) of measurements hypermetabolic, 39% (n = 11) hypometabolic, and the remaining 21% (n = 6) normal. Although REE was well correlated with estimated BMR (r = 0.82, P < 0.0001), estimated BMR was not consistently an adequate predictor of REE. BMR over- or underestimated REE by >10 kcal · kg · day in 15 of 28 (54%) patients. REE was not significantly correlated with severity of liver disease, nutritional status, total energy intake, or gestational age.
Conclusions: Energy expenditure is variable among children with IF and IF-associated liver disease, with approximately 80% of our cohort exhibiting either hypo- or hypermetabolism. Standard estimation equations frequently do not correctly predict individual REE. Longitudinal studies of energy expenditure and body composition may be needed to guide provision of nutrition regimens.
Figures
Similar articles
-
Predicted versus measured resting energy expenditure in patients requiring home parenteral nutrition.Nutrition. 2015 Nov-Dec;31(11-12):1328-32. doi: 10.1016/j.nut.2015.05.002. Epub 2015 Jun 1. Nutrition. 2015. PMID: 26278135
-
A critical view of the use of predictive energy equations for the identification of hypermetabolism in motor neuron disease: A pilot study.Clin Nutr ESPEN. 2023 Oct;57:739-748. doi: 10.1016/j.clnesp.2023.08.017. Epub 2023 Aug 18. Clin Nutr ESPEN. 2023. PMID: 37739732
-
Prediction Equations Underestimate Resting Energy Expenditure in Patients With End-Stage Cystic Fibrosis.Nutr Clin Pract. 2017 Feb;32(1):116-121. doi: 10.1177/0884533616645819. Epub 2016 Jul 10. Nutr Clin Pract. 2017. PMID: 27143650
-
Indirect calorimetry and nutritional problems in clinical practice.Acta Diabetol. 2001;38(1):1-5. doi: 10.1007/s005920170022. Acta Diabetol. 2001. PMID: 11487171 Review.
-
Are Predictive Energy Expenditure Equations Accurate in Cirrhosis?Nutrients. 2019 Feb 4;11(2):334. doi: 10.3390/nu11020334. Nutrients. 2019. PMID: 30720726 Free PMC article. Review.
Cited by
-
Comparison of body composition assessment methods in pediatric intestinal failure.J Pediatr Gastroenterol Nutr. 2014 Jul;59(1):99-105. doi: 10.1097/MPG.0000000000000364. J Pediatr Gastroenterol Nutr. 2014. PMID: 24614122 Free PMC article.
-
Clarifying main nutritional aspects and resting energy expenditure in children with Smith-Magenis syndrome.Eur J Pediatr. 2024 Oct;183(10):4563-4571. doi: 10.1007/s00431-024-05715-z. Epub 2024 Aug 20. Eur J Pediatr. 2024. PMID: 39162735 Free PMC article.
-
Etiology and Management of Pediatric Intestinal Failure: Focus on the Non-Digestive Causes.Nutrients. 2021 Feb 27;13(3):786. doi: 10.3390/nu13030786. Nutrients. 2021. PMID: 33673586 Free PMC article. Review.
-
Necrotizing Enterocolitis and Central Line Associated Blood Stream Infection Are Predictors of Growth Outcomes in Infants with Short Bowel Syndrome.J Pediatr. 2015 Jul;167(1):35-40.e1. doi: 10.1016/j.jpeds.2015.02.053. Epub 2015 Apr 1. J Pediatr. 2015. PMID: 25841540 Free PMC article.
-
Fetal programming of human energy homeostasis brain networks: Issues and considerations.Obes Rev. 2022 Mar;23(3):e13392. doi: 10.1111/obr.13392. Epub 2021 Nov 30. Obes Rev. 2022. PMID: 34845821 Free PMC article. Review.
References
-
- Buchman AL. Etiology and initial management of short bowel syndrome. Gastroenterology. 2006;130:S5–S15. - PubMed
-
- Wilmore DW, Dudrick SJ. Growth and development of an infant receiving all nutrients exclusively by vein. Jama. 1968;203:860–4. - PubMed
-
- Dorney SF, Ament ME, Berquist WE, Vargas JH, Hassall E. Improved survival in very short small bowel of infancy with use of long-term parenteral nutrition. J Pediatr. 1985;107:521–5. - PubMed
-
- Quiros-Tejeira RE, Ament ME, Reyen L, Herzog F, Merjanian M, Olivares-Serrano N, Vargas JH. Long-term parenteral nutritional support and intestinal adaptation in children with short bowel syndrome: a 25-year experience. J Pediatr. 2004;145:157–63. - PubMed
-
- Andorsky DJ, Lund DP, Lillehei CW, Jaksic T, Dicanzio J, Richardson DS, Collier SB, Lo C, Duggan C. Nutritional and other postoperative management of neonates with short bowel syndrome correlates with clinical outcomes. J Pediatr. 2001;139:27–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
