

Diagnosis of covert hepatic encephalopathy without specialized tests
- PMID: 24362049
- PMCID: PMC4063880
- DOI: 10.1016/j.cgh.2013.12.020
Diagnosis of covert hepatic encephalopathy without specialized tests
Abstract
Background & aims: Covert hepatic encephalopathy (CHE) impairs quality of life (QOL) and can be difficult to diagnose. Patient-administered methods that do not require specialized tests or equipment might increase rates of detection. We performed a longitudinal study to determine whether demographic data and responses to a validated QOL questionnaire, the Sickness Impact Profile (SIP), can identify patients with CHE.
Methods: Patients with cirrhosis without prior overt HE were recruited from outpatient liver clinics at the Virginia Commonwealth University Medical Center, from August 2008 through February 2012. We performed cognitive tests on 170 patients (mean age, 55 y; mean model for end-stage liver disease score, 9; 50% with hepatitis C-associated and 11% with alcohol-associated cirrhosis). Patients also were given the SIP questionnaire (136 questions on 12 QOL topics, requiring a yes or no answer) at enrollment, at 6 months, and at 12 months. The proportion of patients that responded "yes" to each question was compared between those with and without CHE. Patient variables (noncognitive), demographics (age, education, sex, alcoholic etiology), and SIP questions that produced different responses between groups were analyzed by logistic regression and receiver operating characteristic analyses.
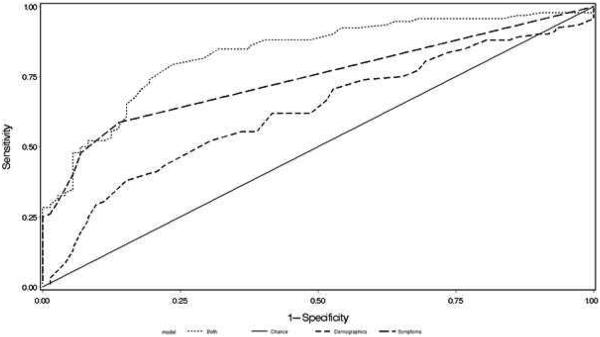
Results: Based on cognitive test results, 93 patients (55%) had CHE when the study began. They had a higher proportion of "yes" responses to 54 questions on the SIP questionnaire, across all categories. We developed a formula to identify patients with CHE based on age, sex, and responses to 4 SIP questions (a SIP CHE score). Baseline SIP CHE scores greater than 0 identified patients with CHE with 80% sensitivity and 79% specificity. Of the 98 patients who returned for the 6-month evaluation, 50% had CHE (the SIP CHE identified these patients with 88% sensitivity). Of the 50 patients who returned for the 12-month evaluation, 32% had CHE (the SIP CHE score identified these patients with 81% sensitivity).
Conclusions: We developed a system to identify patients with CHE based on age, sex, and responses to 4 SIP questions; this formula identified patients with CHE with more than 80% sensitivity over a 12-month period after the initial enrollment. Patient-administered CHE screening strategies that do not include specialized tests could increase the detection of CHE and improve therapy.
Keywords: Cirrhosis; Cognition; HRQOL; Minimal Hepatic Encephalopathy; Psychometric Tests; Sickness Impact Profile.
Copyright © 2014 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Kappus MR, Bajaj JS. Covert hepatic encephalopathy: not as minimal as you might think. Clin Gastroenterol Hepatol. 2012;10:1208–1219. - PubMed
-
- Ortiz M, Jacas C, Cordoba J. Minimal hepatic encephalopathy: diagnosis, clinical significance and recommendations. J Hepatol. 2005;42:S45–53. Suppl. - PubMed
-
- Bajaj JS, Etemadian A, Hafeezullah M, Saeian K. Testing for minimal hepatic encephalopathy in the United States: An AASLD survey. Hepatology. 2007;45:833–834. - PubMed
-
- Prasad S, Dhiman RK, Duseja A, Chawla YK, Sharma A, Agarwal R. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology. 2007;45:549–559. - PubMed
-
- Kanwal F, Gralnek IM, Hays RD, Zeringue A, Durazo F, Han SB, Saab S, et al. Health-related quality of life predicts mortality in patients with advanced chronic liver disease. Clin Gastroenterol Hepatol. 2009;7:793–799. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
