

Epidemiology of human respiratory viruses in children with acute respiratory tract infections in Jinan, China
- PMID: 24363757
- PMCID: PMC3865640
- DOI: 10.1155/2013/210490
Epidemiology of human respiratory viruses in children with acute respiratory tract infections in Jinan, China
Abstract
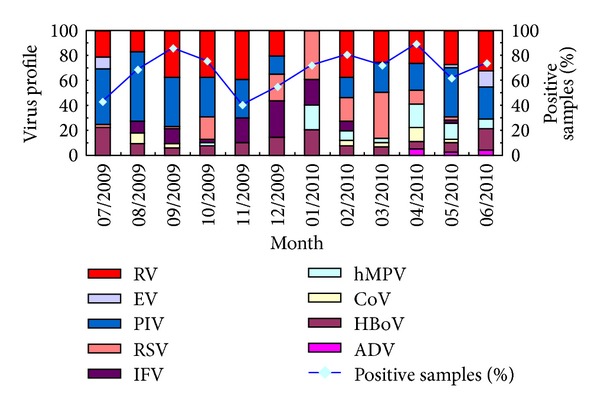
The viral etiologies of UTRIs and LTRIs in children in Jinan city were investigated between July 2009 and June 2010. Nasal and throat swabs were collected from 397 children with URTIs and bronchoalveolar lavage fluid specimens were collected from 323 children with LRTIs. RT-PCR/PCR was used to examine all samples for IFV, PIV, RSV, RV, hMPV, HBoV, CoV, ADV, RSV, and EV. Viral pathogens were detected in 47.10% of URTI samples and 66.57% samples, and the incidence of viral coinfection was 5.29% and 21.05%, respectively. IFV was the most common virus in URTIs, with a detection rate of 19.40%, followed by PIV (10.83%), RV (10.58%), and EV (6.30%). For LRTIs, PIV and RV were both detected in 27% of samples, followed by RSV (9.91%), HBoV (8.36%), IFV (5.57%), and hMPV (5.57%). RSV and HBoV were more prevalent in the youngest children of no more than six months. Meanwhile, RV, PIV, and RSV were the most frequent viruses combined with bacterial pathogens in LRTIs. In conclusion, the spectrum of respiratory virus infections in URTIs and LRTIs differed in terms of the most common pathogens, seasonal distribution, and coinfection rate.
Figures



References
-
- Demers A-M, Morency P, Mberyo-Yaah F, et al. Risk factors for mortality among children hospitalized because of acute respiratory infections in Bangui, Central African Republic. Pediatric Infectious Disease Journal. 2000;19(5):424–432. - PubMed
-
- Garbino J, Gerbase MW, Wunderli W, et al. Respiratory viruses and severe lower respiratory tract complications in hospitalized patients. Chest. 2004;125(3):1033–1039. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
