

Increased risk for chronic comorbid disorders in patients with inflammatory arthritis: a population based study
- PMID: 24364915
- PMCID: PMC3909051
- DOI: 10.1186/1471-2296-14-199
Increased risk for chronic comorbid disorders in patients with inflammatory arthritis: a population based study
Abstract
Background: Studies determining the development of a wide variety of different comorbid disorders in inflammatory arthritis (IA) patients are scarce, however, this knowledge could be helpful in optimising preventive care in IA patients. The aim of this study is to establish the risk that new chronic comorbid disorders in newly diagnosed patients with IA in a primary care setting are developed.
Methods: This is a nested-case-control study from 2001-2010 using data from electronic medical patient records in general practice. In total, 3,354 patients with newly diagnosed IA were selected. Each patient was matched with two control patients of the same age and sex in the same general practice. The development of 121 chronic comorbid disorders of index and control patients was compared using Cox regression.
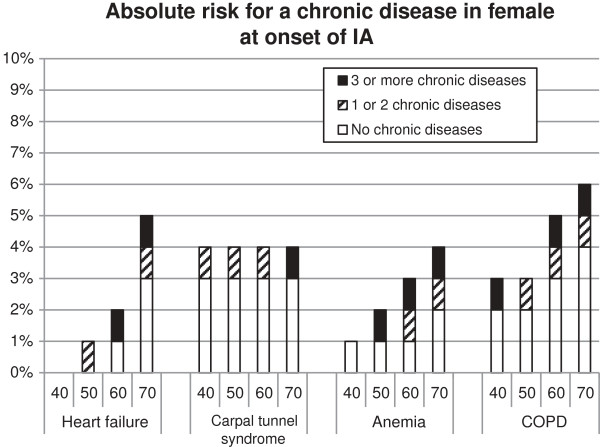
Results: After a median follow-up period of 2.8 years, 56% of the IA-patients had developed at least one chronic comorbid disorder after the onset of IA, compared to 46% of the control patients (p < 0.05). The most frequent developed comorbid disorders after the onset of IA were of cardiovascular (23%), and musculoskeletal (17%) origin. The highest hazard ratios (HRs) were found for anaemia (HR 2.0 [95% CI: 1.4-2.7]) osteoporosis (HR 1.9 [1.4-2.4]), and COPD (HR 1.8 [1.4-2.3]).
Conclusion: Patients with IA developed more chronic comorbid disorders after the onset of IA than one might expect based on age and sex. Since comorbidity has a large impact on the disease course, quality of life, and possibly on treatment itself, prevention of comorbidity should be one of the main targets in the treatment of IA patients.
Figures


References
-
- Scott DL, Symmons DP, Coulton BL, Popert AJ. Long-term outcome of treating rheumatoid arthritis: results after 20 years. Lancet. 1987;14:1108–1111. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
