

In-vitro renal epithelial cell infection reveals a viral kidney tropism as a potential mechanism for acute renal failure during Middle East Respiratory Syndrome (MERS) Coronavirus infection
- PMID: 24364985
- PMCID: PMC3878046
- DOI: 10.1186/1743-422X-10-359
In-vitro renal epithelial cell infection reveals a viral kidney tropism as a potential mechanism for acute renal failure during Middle East Respiratory Syndrome (MERS) Coronavirus infection
Abstract
Background: The Middle East Respiratory Syndrome Coronavirus (MERS-CoV) causes symptoms similar to Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV), yet involving an additional component of acute renal failure (ARF) according to several published case reports. Impairment of the kidney is not typically seen in Coronavirus infections. The role of kidney infection in MERS is not understood.
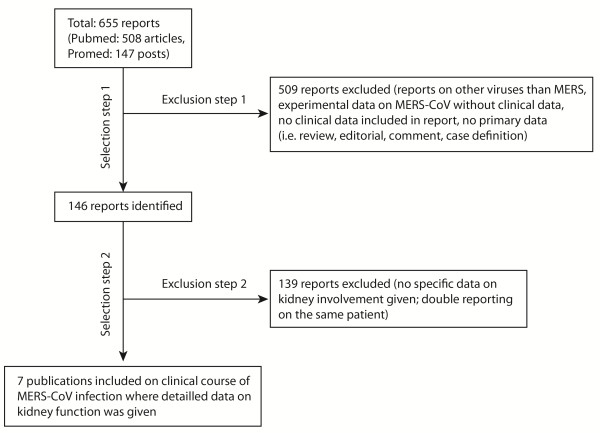
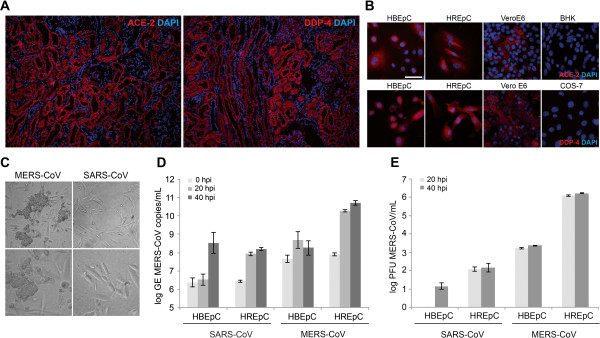
Findings: A systematic review of communicated and peer-reviewed case reports revealed differences in descriptions of kidney involvement in MERS versus SARS patients. In particular, ARF in MERS patients occurred considerably earlier after a median time to onset of 11 days (SD ±2,0 days) as opposed to 20 days for SARS, according to the literature. In-situ histological staining of the respective cellular receptors for MERS- and SARS-Coronavirus showed highly similar staining patterns with a focus of a receptor-specific signal in kidney epithelial cells. Comparative infection experiments with SARS- and MERS-CoV in primary human kidney cells versus primary human bronchial epithelial cells showed cytopathogenic infection only in kidney cells, and only if infected with MERS-CoV. Kidney epithelial cells produced almost 1000-fold more infectious MERS-CoV progeny than bronchial epithelial cells, while only a small difference was seen between cell types when infected with SARS-CoV.
Conclusion: Epidemiological studies should analyze kidney impairment and its characteristics in MERS-CoV. Virus replication in the kidney with potential shedding in urine might constitute a way of transmission, and could explain untraceable transmission chains leading to new cases. Individual patients might benefit from early induction of renoprotective treatment.
Figures
References
-
- Drosten C, Seilmaier M, Corman VM, Hartmann W, Scheible G, Sack S, Guggemos W, Kallies R, Muth D, Junglen S. et al. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis. 2013;10:745–751. doi: 10.1016/S1473-3099(13)70154-3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
