

Prognostic importance of pathophysiologic markers in patients with heart failure and preserved ejection fraction
- PMID: 24365774
- PMCID: PMC5947992
- DOI: 10.1161/CIRCHEARTFAILURE.113.000854
Prognostic importance of pathophysiologic markers in patients with heart failure and preserved ejection fraction
Abstract
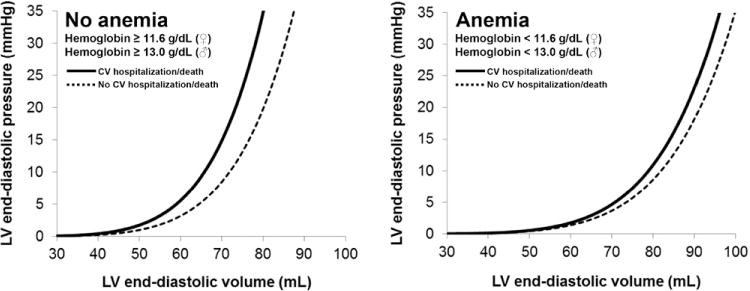
Background: Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous syndrome associated with multiple pathophysiologic abnormalities, including left ventricular (LV) diastolic dysfunction, longitudinal LV systolic dysfunction, abnormal ventricular-arterial coupling, pulmonary hypertension, and right ventricular (RV) remodeling/dysfunction. However, the relative prognostic significance of each of these pathophysiologic abnormalities in HFpEF is unknown.
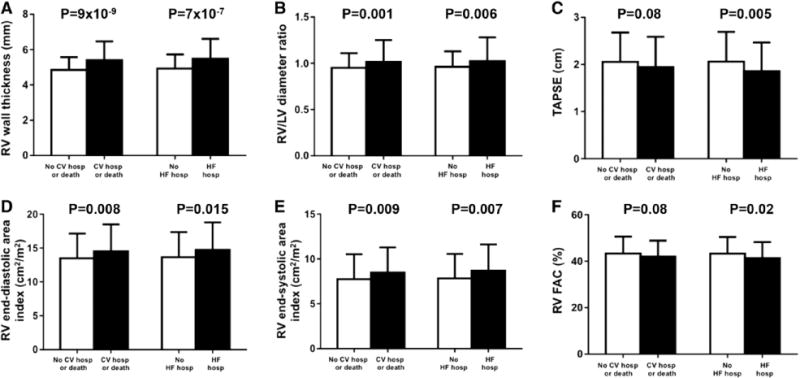
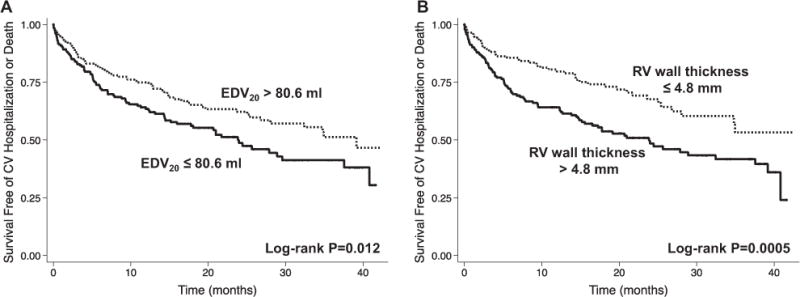
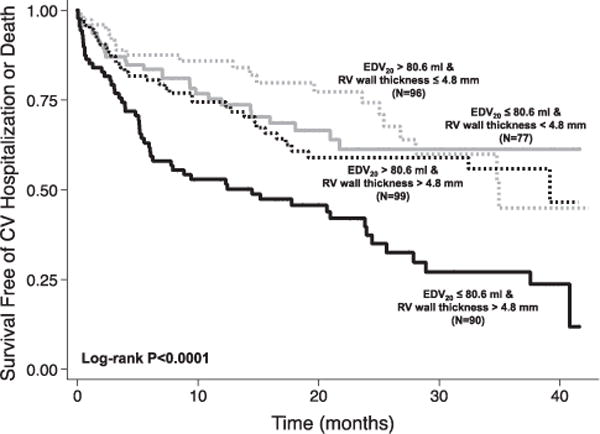
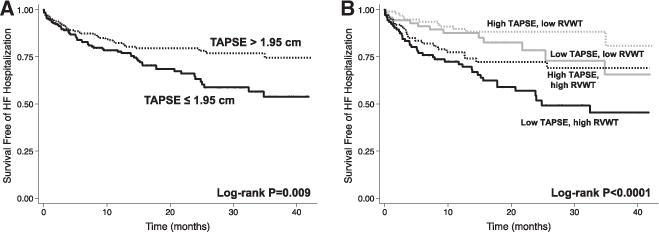
Methods and results: We prospectively studied 419 patients with HFpEF using echocardiography and sphygmomanometry to assess HFpEF pathophysiologic markers. Cox proportional hazards analyses were used to determine the associations between pathophysiologic markers and outcomes. Mean age was 65±12 years; 62% were women; 39% were black; comorbidities were common; and study participants met published criteria for HFpEF. RV abnormalities were frequent: 28% had abnormal tricuspid annular plane systolic excursion, 15% had reduced RV fractional area change, and 34% had RV hypertrophy. During a median follow-up time of 18 months, 102 (24%) were hospitalized for HF and 175 (42%) experienced the composite end point of cardiovascular hospitalization or death. Decreased LV compliance, measured as reduced LV end-diastolic volume at an idealized LV end-diastolic pressure of 20 mm Hg (EDV20), and RV remodeling, as indicated by increased RV wall thickness, were the 2 pathophysiologic markers most predictive of worse outcomes: adjusted hazard ratio per 1 SD decrease in EDV20=1.39 (95% confidence interval [CI], 1.10-1.75; P=0.006), and hazard ratio per 1 SD increase in RV wall thickness=1.37 (95% CI, 1.16-1.61; P<0.001). These associations persisted after additional adjustment for markers of HF severity. By contrast, markers of LV relaxation, longitudinal LV systolic dysfunction, and ventricular-arterial coupling were not significantly associated with adverse outcomes.
Conclusions: In patients with HFpEF, reduced LV compliance and RV remodeling are the strongest pathophysiologic predictors of adverse outcomes.
Keywords: heart failure, diastolic; heart ventricles; ventricular dysfunction, right.
Figures
References
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–269. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Campbell RT, Jhund PS, Castagno D, Hawkins NM, Petrie MC, McMurray JJ. What have we learned about patients with heart failure and preserved ejection fraction from DIG-PEF, CHARM-preserved, and I-PRESERVE? J Am Coll Cardiol. 2012;60:2349–2356. - PubMed
-
- Setaro JF, Zaret BL, Schulman DS, Black HR, Soufer R. Usefulness of verapamil for congestive heart failure associated with abnormal left ventricular diastolic filling and normal left ventricular systolic performance. Am J Cardiol. 1990;66:981–986. - PubMed
-
- Aronow WS, Ahn C, Kronzon I. Effect of propranolol versus no propranolol on total mortality plus nonfatal myocardial infarction in older patients with prior myocardial infarction, congestive heart failure, and left ventricular ejection fraction > or = 40% treated with diuretics plus angiotensin-converting enzyme inhibitors. Am J Cardiol. 1997;80:207–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
