

Race/Ethnicity, disability, and medication adherence among medicare beneficiaries with heart failure
- PMID: 24366395
- PMCID: PMC3965752
- DOI: 10.1007/s11606-013-2692-x
Race/Ethnicity, disability, and medication adherence among medicare beneficiaries with heart failure
Abstract
Background: Recent and national data on adherence to heart failure drugs are limited, particularly among the disabled and some small minority groups, such as Native Americans and Hispanics.
Objective: We compare medication adherence among Medicare patients with heart failure, by disability status, race/ethnicity, and income.
Design: Observational study.
Setting: US Medicare Parts A, B, and D data, 5% random sample, 2007-2009.
Participants: 149,893 elderly Medicare beneficiaries and 21,204 disabled non-elderly beneficiaries.
Main measures: We examined 5% of Medicare fee-for-service beneficiaries with heart failure in 2007-2009. The main outcome was 1-year adherence to one of three therapeutic classes: β-blockers, diuretics, and angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin II receptor blockers (ARBs). Adherence was defined as having prescriptions in possession for ≥ 75% of days.
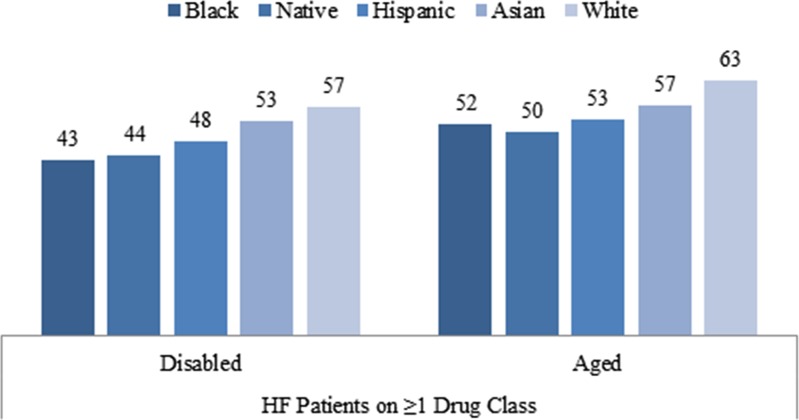
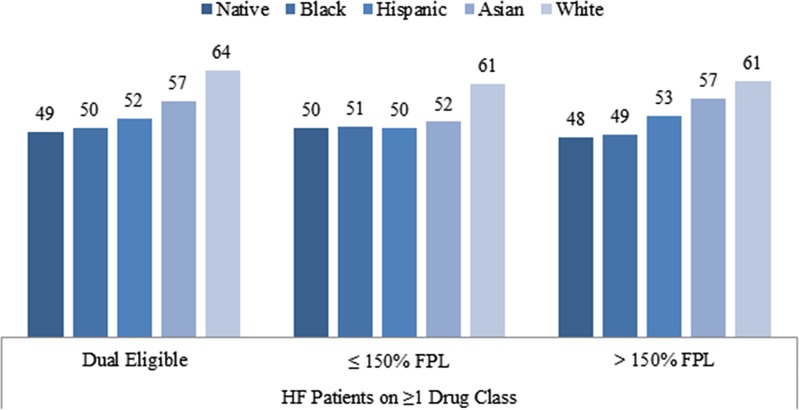
Key results: Among aged beneficiaries, 1-year adherences to at least one heart failure drug were 63%, 57%, 53%, 50%, and 52% for Whites, Asians, Hispanics, Native Americans and Blacks, respectively; among the disabled, 1-year adherence was worse for each group: 57%, 53%, 48%, 44% and 43% respectively. The racial/ethnic difference persisted after adjustment for age, gender, income, drug coverage, location and health status. Patterns of adherence were similar among beneficiaries on all three therapeutic classes. Among beneficiaries with close-to-full drug coverage, minorities were still less likely to adhere relative to Whites, OR = 0.61 (95% CI 0.58-0.64) for Hispanics, OR = 0.59 (95% CI 0.57-0.62) for Blacks and OR = 0.57 (95% CI 0.47-0.68) for Native Americans.
Conclusion: After the implementation of Medicare Part D, adherence to heart failure drugs remains problematic, especially among disabled and minority beneficiaries, including Native Americans, Blacks, and Hispanics. Even among those with close-to-full drug coverage, racial differences remain, suggesting that policies simply relying on cost reduction cannot eliminate racial differences.
Figures
Comment in
-
Capsule commentary on Zhang et al., Race/ethnicity, disability, and medication adherence among medicare beneficiaries with heart failure.J Gen Intern Med. 2014 Apr;29(4):648. doi: 10.1007/s11606-013-2736-2. J Gen Intern Med. 2014. PMID: 24481685 Free PMC article. No abstract available.
References
-
- Heart and Stroke Statistical Update. Dallas: American Heart Association 2006; 2006.
-
- Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):1977–2016. doi: 10.1161/CIRCULATIONAHA.109.192064. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
