

Neonatal hyperbilirubinemia and Rhesus disease of the newborn: incidence and impairment estimates for 2010 at regional and global levels
- PMID: 24366465
- PMCID: PMC3873706
- DOI: 10.1038/pr.2013.208
Neonatal hyperbilirubinemia and Rhesus disease of the newborn: incidence and impairment estimates for 2010 at regional and global levels
Abstract
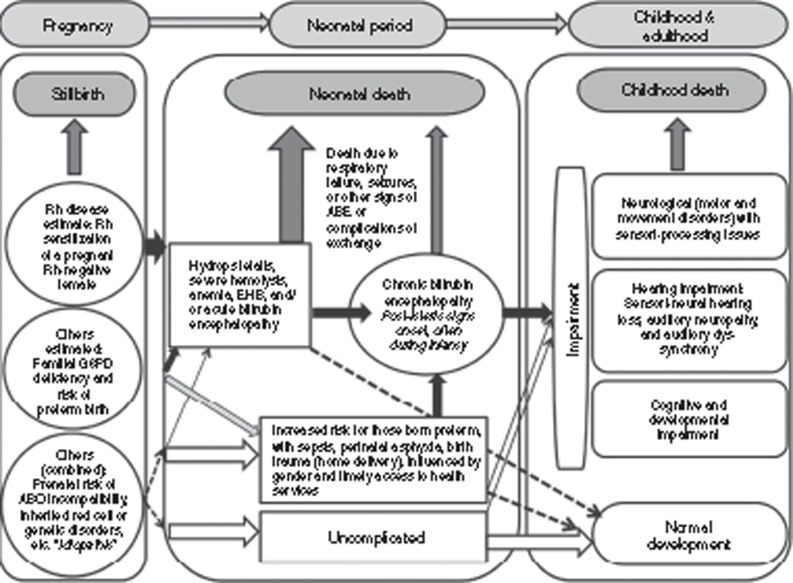
Background: Rhesus (Rh) disease and extreme hyperbilirubinemia (EHB) result in neonatal mortality and long-term neurodevelopmental impairment, yet there are no estimates of their burden.
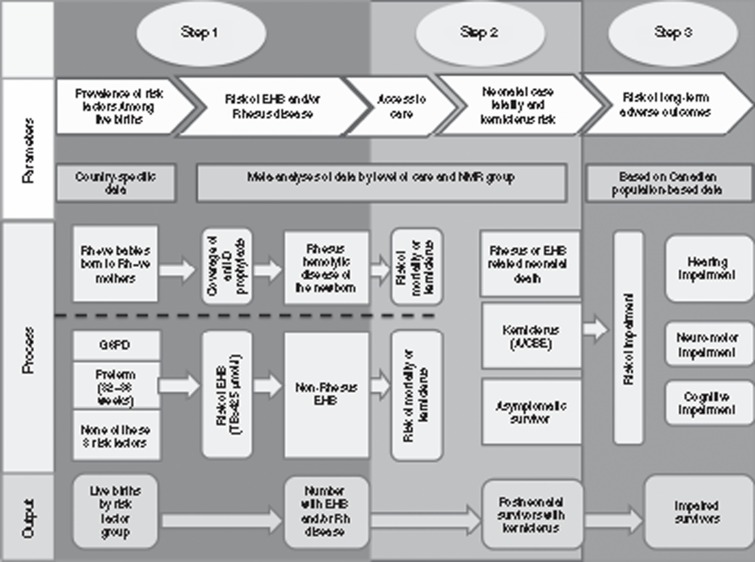
Methods: Systematic reviews and meta-analyses were undertaken of national prevalence, mortality, and kernicterus due to Rh disease and EHB. We applied a compartmental model to estimate neonatal survivors and impairment cases for 2010.
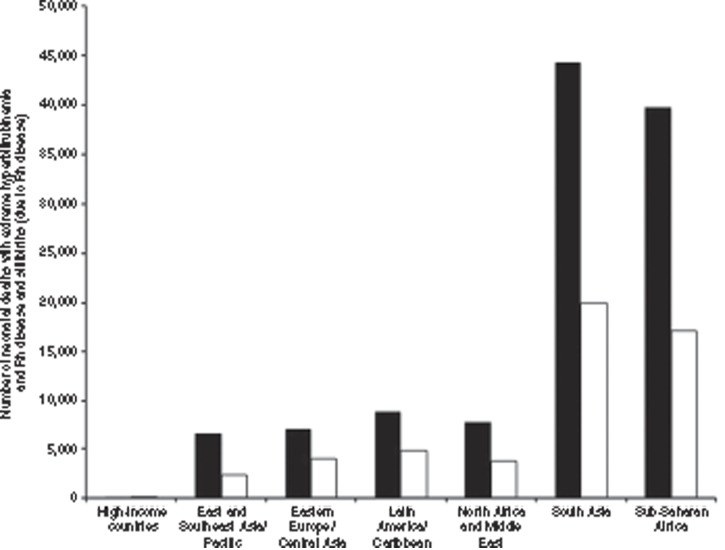
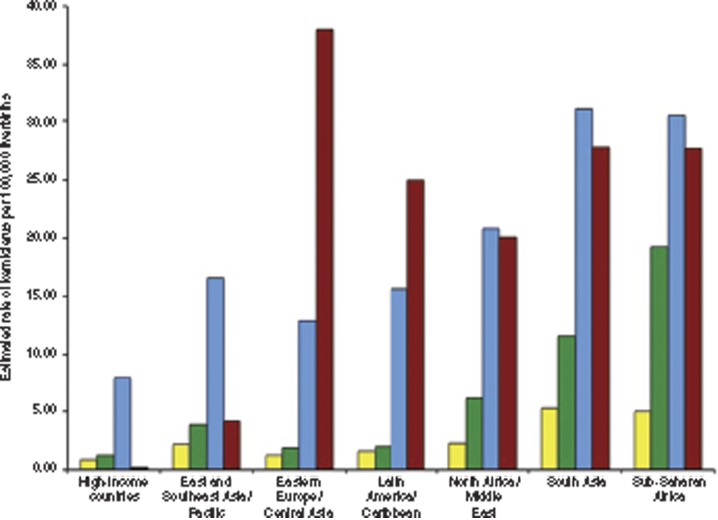
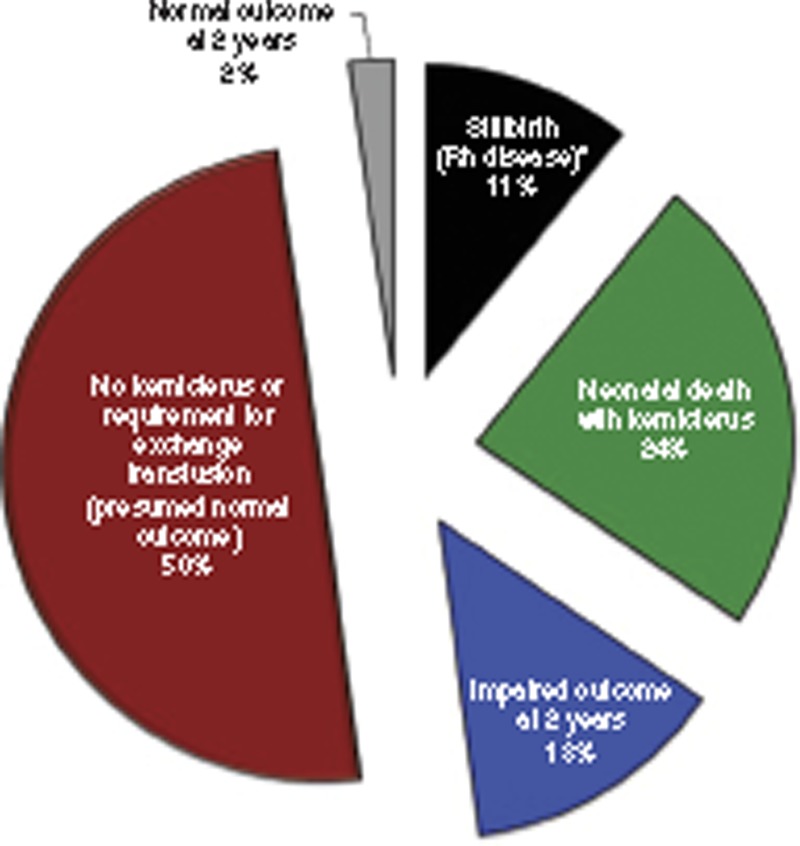
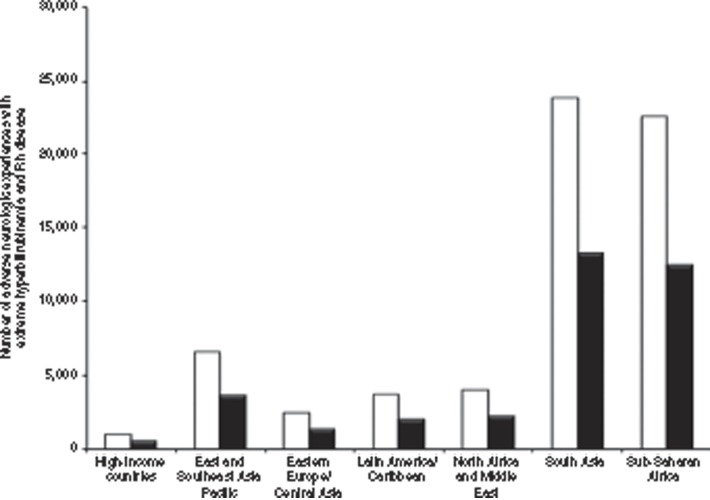
Results: Twenty-four million (18% of 134 million live births ≥ 32 wk gestational age from 184 countries; uncertainty range: 23-26 million) were at risk for neonatal hyperbilirubinemia-related adverse outcomes. Of these, 480,700 (0.36%) had either Rh disease (373,300; uncertainty range: 271,800-477,500) or developed EHB from other causes (107,400; uncertainty range: 57,000-131,000), with a 24% risk for death (114,100; uncertainty range: 59,700-172,000), 13% for kernicterus (75,400), and 11% for stillbirths. Three-quarters of mortality occurred in sub-Saharan Africa and South Asia. Kernicterus with Rh disease ranged from 38, 28, 28, and 25/100,000 live births for Eastern Europe/Central Asian, sub-Saharan African, South Asian, and Latin American regions, respectively. More than 83% of survivors with kernicterus had one or more impairments.
Conclusion: Failure to prevent Rh sensitization and manage neonatal hyperbilirubinemia results in 114,100 avoidable neonatal deaths and many children grow up with disabilities. Proven solutions remain underused, especially in low-income countries.
Figures
References
-
- American Academy of Pediatrics Subcommittee on H. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114:297–316. - PubMed
-
- Maisels MJ, Bhutani VK, Bogen D, Newman TB, Stark AR, Watchko JF. Hyperbilirubinemia in the newborn infant > or =35 weeks' gestation: an update with clarifications. Pediatrics. 2009;124:1193–8. - PubMed
-
- Bhutani VK, Stark AR, Lazzeroni LC, et al. Initial Clinical Testing Evaluation and Risk Assessment for Universal Screening for Hyperbilirubinemia Study Group Predischarge screening for severe neonatal hyperbilirubinemia identifies infants who need phototherapy. J Pediatr. 2013;162:477–482.e1. - PubMed
-
- Keren R, Tremont K, Luan X, Cnaan A. Visual assessment of jaundice in term and late preterm infants. Arch Dis Child Fetal Neonatal Ed. 2009;94:F317–22. - PubMed
-
- Johnson LH, Bhutani VK, Brown AK. System-based approach to management of neonatal jaundice and prevention of kernicterus. J Pediatr. 2002;140:396–403. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
