

Outcome of pediatric acute myeloid leukemia patients receiving intensive care in the United States
- PMID: 24366507
- PMCID: PMC4407366
- DOI: 10.1097/PCC.0000000000000042
Outcome of pediatric acute myeloid leukemia patients receiving intensive care in the United States
Abstract
Objective: Children with acute myeloid leukemia are at risk for sepsis and organ failure. Outcomes associated with intensive care support have not been studied in a large pediatric acute myeloid leukemia population. Our objective was to determine hospital mortality of pediatric acute myeloid leukemia patients requiring intensive care.
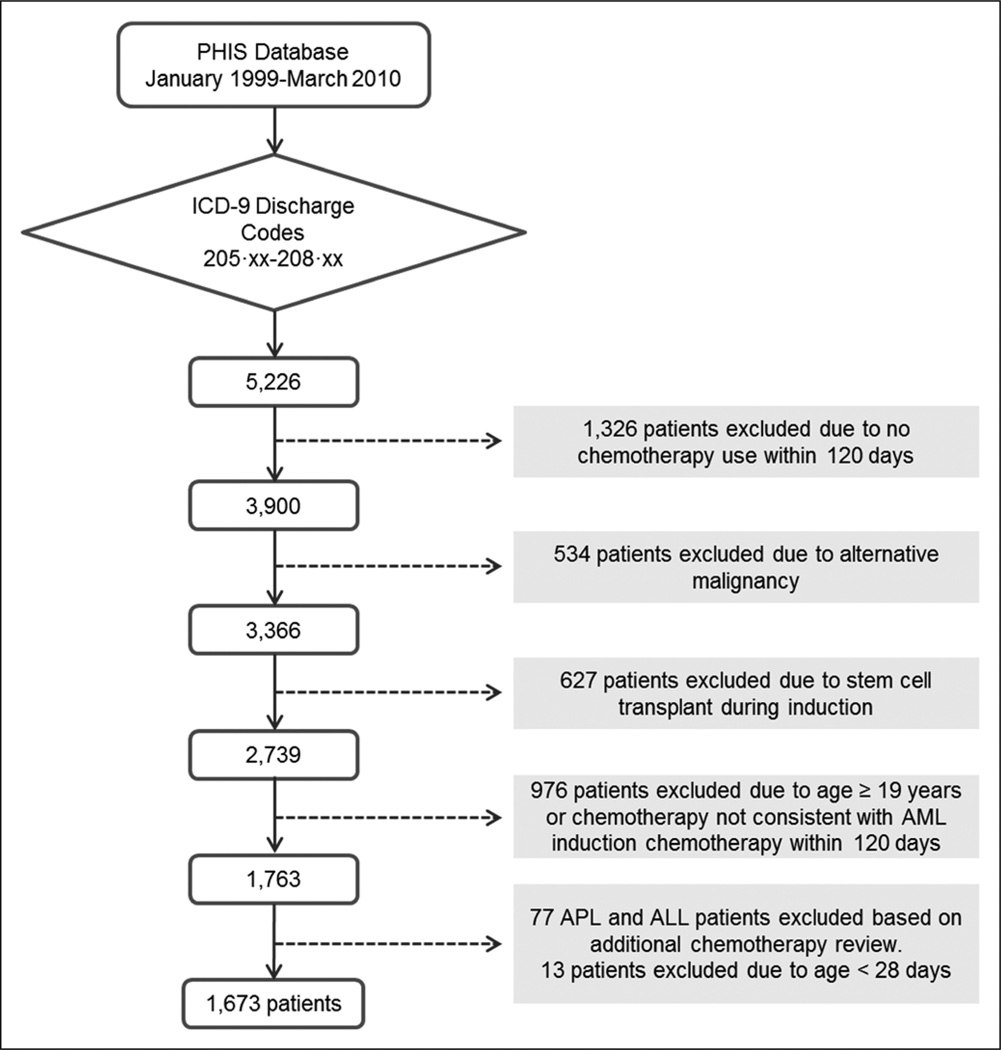
Design: Retrospective cohort study of children hospitalized between 1999 and 2010. Use of intensive care was defined by utilization of specific procedures and resources. The primary endpoint was hospital mortality.
Setting: Forty-three children's hospitals contributing data to the Pediatric Health Information System database.
Patients: Patients who are newly diagnosed with acute myeloid leukemia and who are 28 days through 18 years old (n = 1,673) hospitalized any time from initial diagnosis through 9 months following diagnosis or until stem cell transplant. A reference cohort of all nononcology pediatric admissions using the same intensive care resources in the same time period (n = 242,192 admissions) was also studied.
Interventions: None.
Measurements and main results: One-third of pediatric patients with acute myeloid leukemia (553 of 1,673) required intensive care during a hospitalization within 9 months of diagnosis. Among intensive care admissions, mortality was higher in the acute myeloid leukemia cohort compared with the nononcology cohort (18.6% vs 6.5%; odds ratio, 3.23; 95% CI, 2.64-3.94). However, when sepsis was present, mortality was not significantly different between cohorts (21.9% vs 19.5%; odds ratio, 1.17; 95% CI, 0.89-1.53). Mortality was consistently higher for each type of organ failure in the acute myeloid leukemia cohort versus the nononcology cohort; however, mortality did not exceed 40% unless there were four or more organ failures in the admission. Mortality for admissions requiring intensive care decreased over time for both cohorts (23.7% in 1999-2003 vs 16.4% in 2004-2010 in the acute myeloid leukemia cohort, p = 0.0367; and 7.5% in 1999-2003 vs 6.5% in 2004-2010 in the nononcology cohort, p < 0.0001).
Conclusions: Pediatric patients with acute myeloid leukemia frequently required intensive care resources, with mortality rates substantially lower than previously reported. Mortality also decreased over the time studied. Pediatric acute myeloid leukemia patients with sepsis who required intensive care had a mortality comparable to children without oncologic diagnoses; however, overall mortality and mortality for each category of organ failure studied was higher for the acute myeloid leukemia cohort compared with the nononcology cohort.
Figures
References
-
- Creutzig U, Zimmermann M, Reinhardt D, et al. Early deaths and treatment-related mortality in children undergoing therapy for acute myeloid leukemia: Analysis of the multicenter clinical trials AML-BFM 93 and AML-BFM 98. J Clin Oncol. 2004;22:4384–4393. - PubMed
-
- Riley LC, Hann IM, Wheatley K, et al. Treatment-related deaths during induction and first remission of acute myeloid leukaemia in children treated on the Tenth Medical Research Council acute myeloid leukaemia trial (MRC AML10). The MCR Childhood Leukaemia Working Party. Br J Haematol. 1999;106:436–444. - PubMed
-
- Rubnitz JE, Lensing S, Zhou Y, et al. Death during induction therapy and first remission of acute leukemia in childhood: The St. Jude experience. Cancer. 2004;101:1677–1684. - PubMed
-
- Slats AM, Egeler RM, van der Does-van den Berg A, et al. Causes of death–other than progressive leukemia–in childhood acute lymphoblastic (ALL) and myeloid leukemia (AML): The Dutch Childhood Oncology Group experience. Leukemia. 2005;19:537–544. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
