

The neuropathology of sport
- PMID: 24366527
- PMCID: PMC4255282
- DOI: 10.1007/s00401-013-1230-6
The neuropathology of sport
Abstract
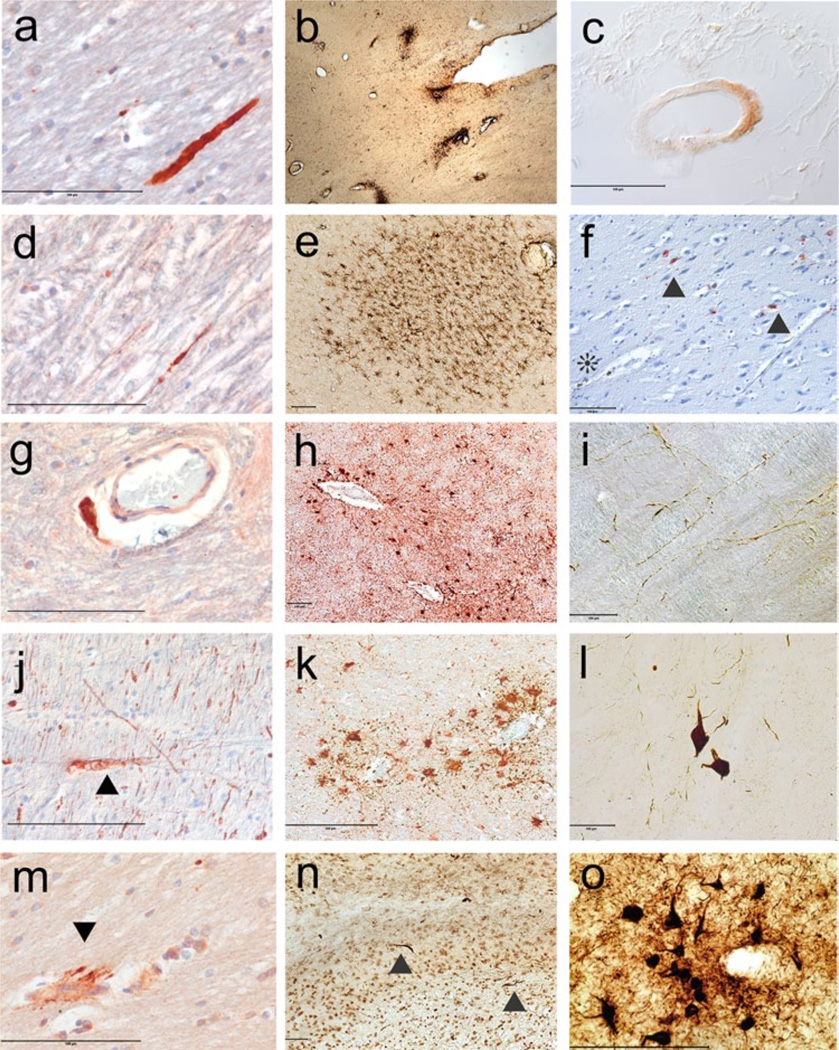
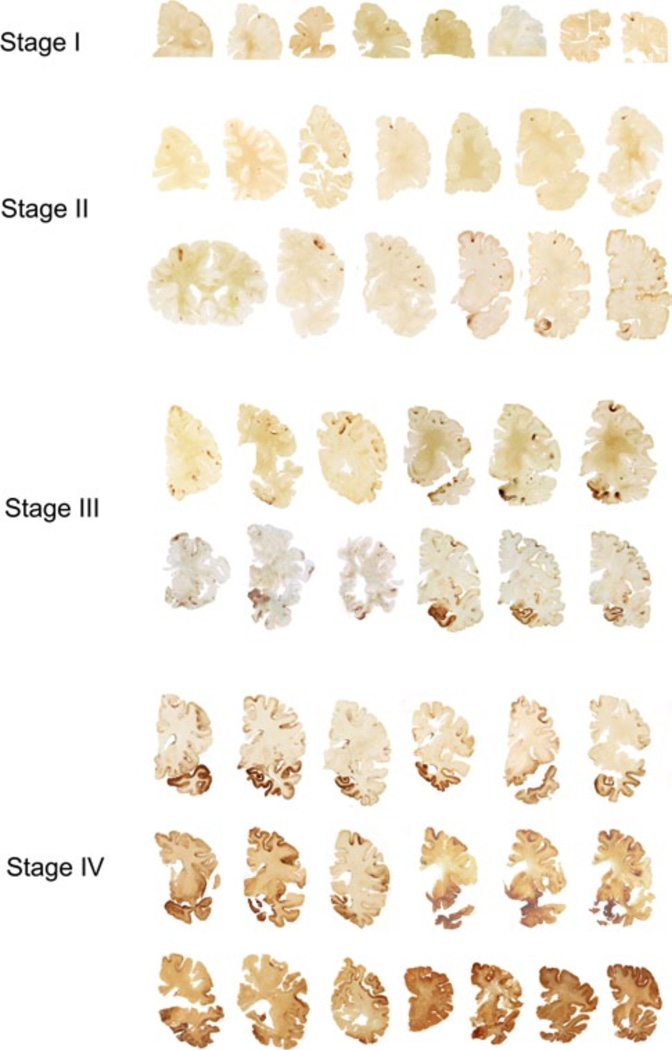
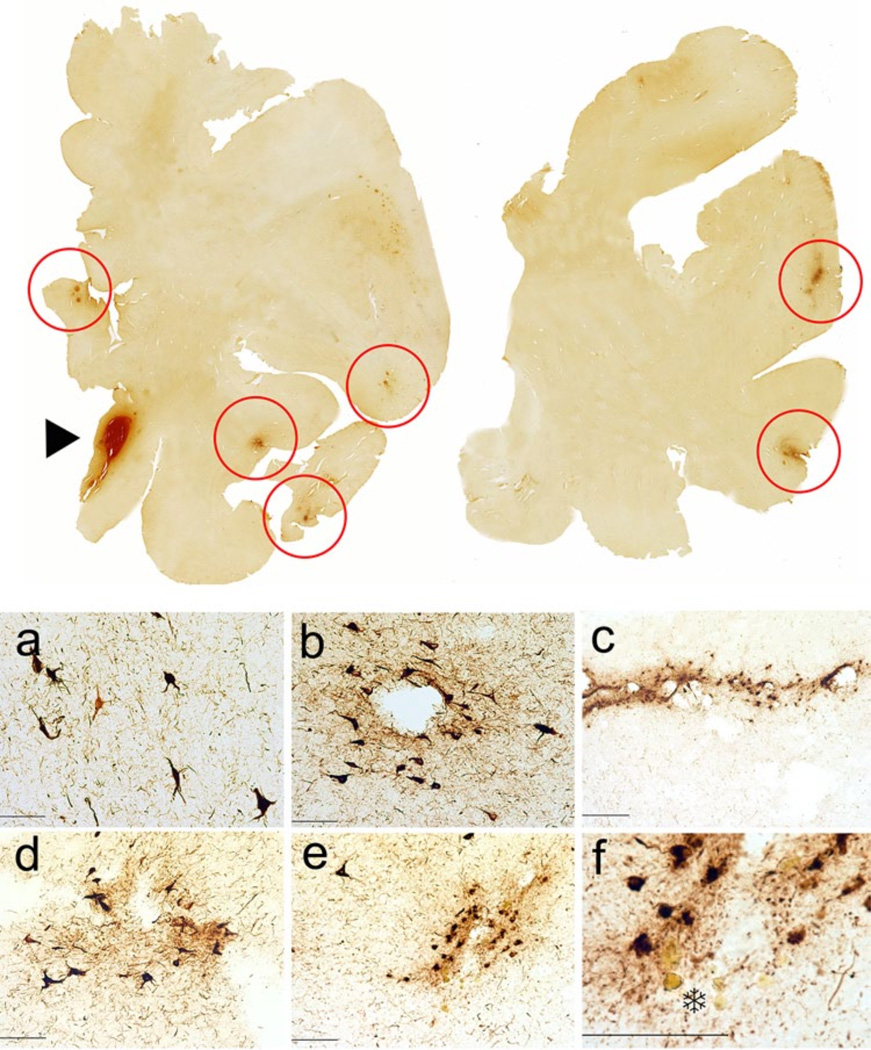
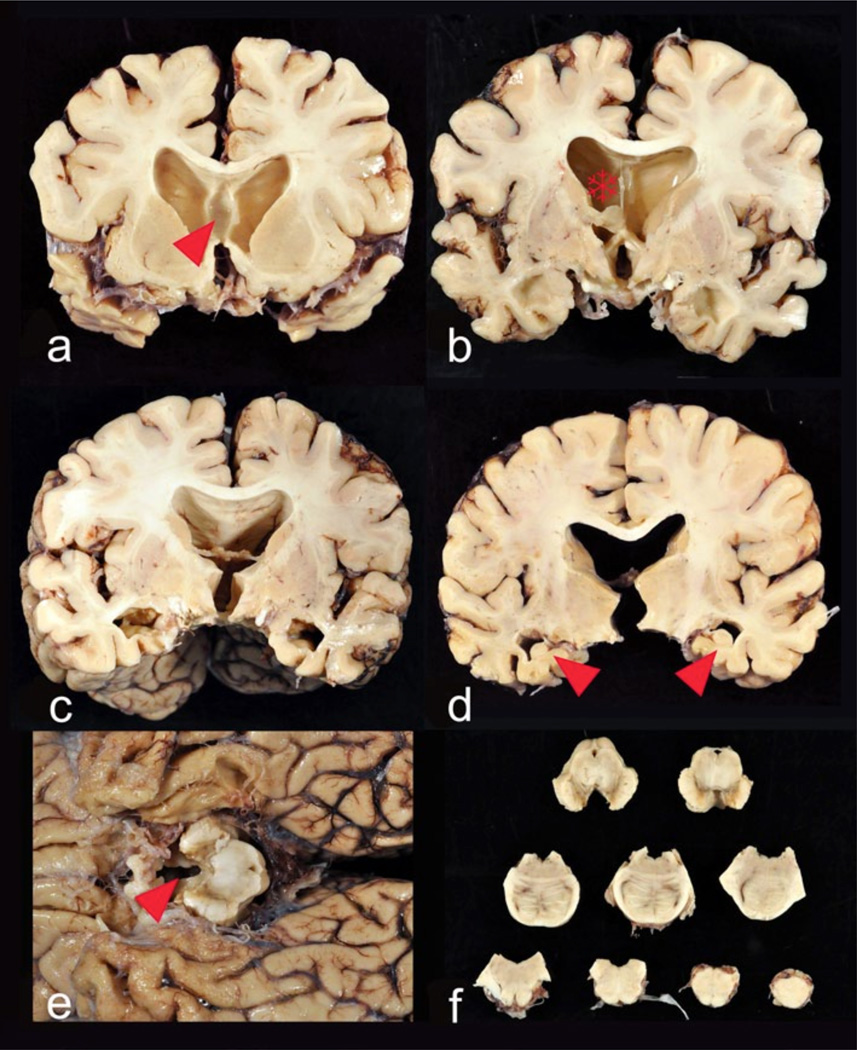
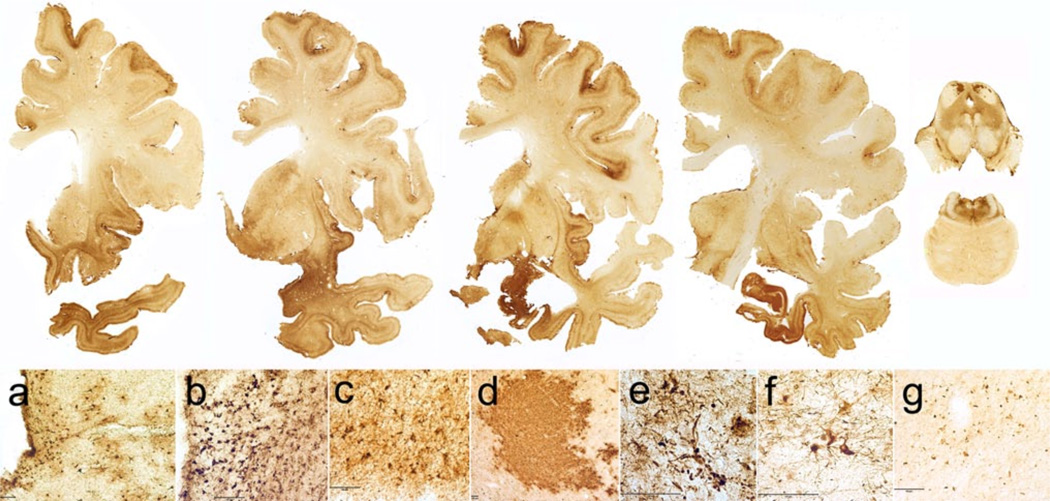
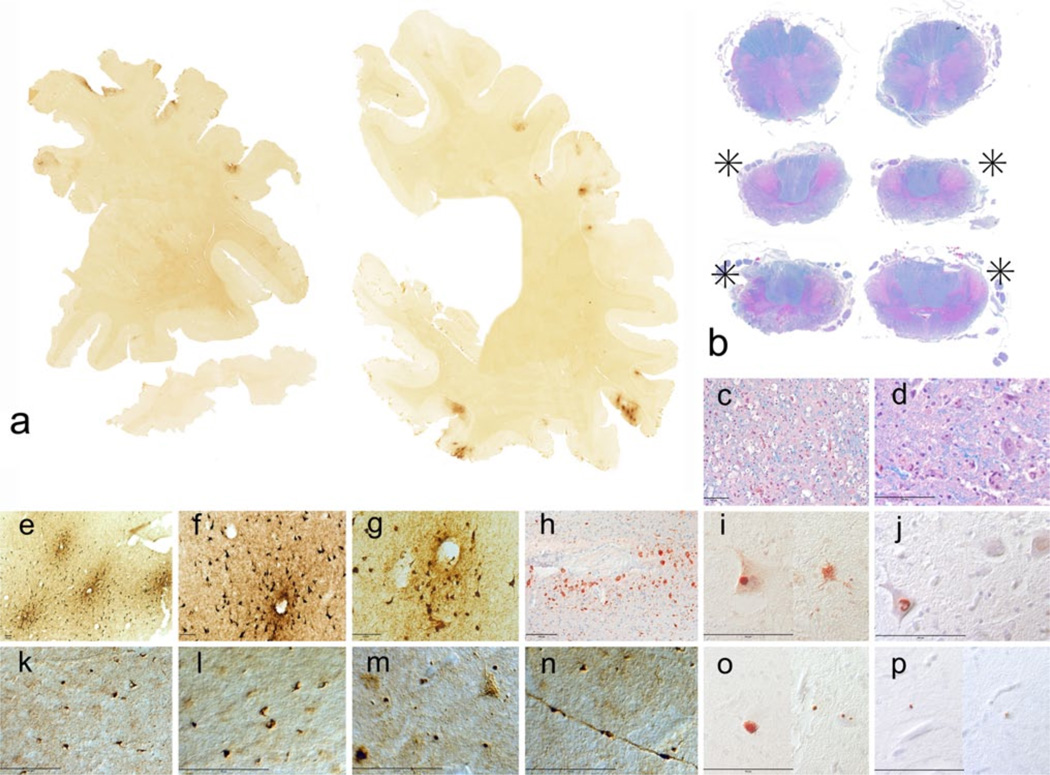
The benefits of regular exercise, physical fitness and sports participation on cardiovascular and brain health are undeniable. Physical activity reduces the risk for cardiovascular disease, type 2 diabetes, hypertension, obesity, and stroke, and produces beneficial effects on cholesterol levels, antioxidant systems, inflammation, and vascular function. Exercise also enhances psychological health, reduces age-related loss of brain volume, improves cognition, reduces the risk of developing dementia, and impedes neurodegeneration. Nonetheless, the play of sports is associated with risks, including a risk for mild TBI (mTBI) and, rarely, catastrophic traumatic injury and death. There is also growing awareness that repetitive mTBIs, such as concussion and subconcussion, can occasionally produce persistent cognitive, behavioral, and psychiatric problems as well as lead to the development of a neurodegeneration, chronic traumatic encephalopathy (CTE). In this review, we summarize the beneficial aspects of sports participation on psychological, emotional, physical and cognitive health, and specifically analyze some of the less common adverse neuropathological outcomes, including concussion, second-impact syndrome, juvenile head trauma syndrome, catastrophic sudden death, and CTE. CTE is a latent neurodegeneration clinically associated with behavioral changes, executive dysfunction and cognitive impairments, and pathologically characterized by frontal and temporal lobe atrophy, neuronal and axonal loss, and abnormal deposits of paired helical filament (PHF)-tau and 43 kDa TAR deoxyribonucleic acid (DNA)-binding protein (TDP-43). CTE often occurs as a sole diagnosis, but may be associated with other neurodegenerative disorders, including motor neuron disease (CTE-MND). Although the incidence and prevalence of CTE are not known, CTE has been reported most frequently in American football players and boxers. Other sports associated with CTE include ice hockey, professional wrestling, soccer, rugby, and baseball.
Figures
References
-
- Ang ET, Dawe GS, Wong PT, Moochhala S, Ng YK. Alterations in spatial learning and memory after forced exercise. Brain Res. 2006;1113(1):186–193. - PubMed
-
- Ang ET, Gomez-Pinilla F. Potential therapeutic effects of exercise to the brain. Curr Med Chem. 2007;14(24):2564–2571. - PubMed
-
- Anthony IC, Norrby KE, Dingwall T, Carnie FW, Millar T, Arango JC, Robertson R, Bell JE. Predisposition to accelerated Alzheimer-related changes in the brains of human immunodeficiency virus negative opiate abusers. Brain. 2010;133(12):3685–3698. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
