

Review
doi: 10.1161/JAHA.113.000473.
Contemporary cardiovascular imaging methods for the assessment of at-risk myocardium
Affiliations
- PMID: 24366853
- PMCID: PMC3959708
- DOI: 10.1161/JAHA.113.000473
Item in Clipboard
Review
Contemporary cardiovascular imaging methods for the assessment of at-risk myocardium
J Am Heart Assoc.
.
No abstract available
Keywords: area at risk; diagnosis; imaging; myocardial infarction.
Figures
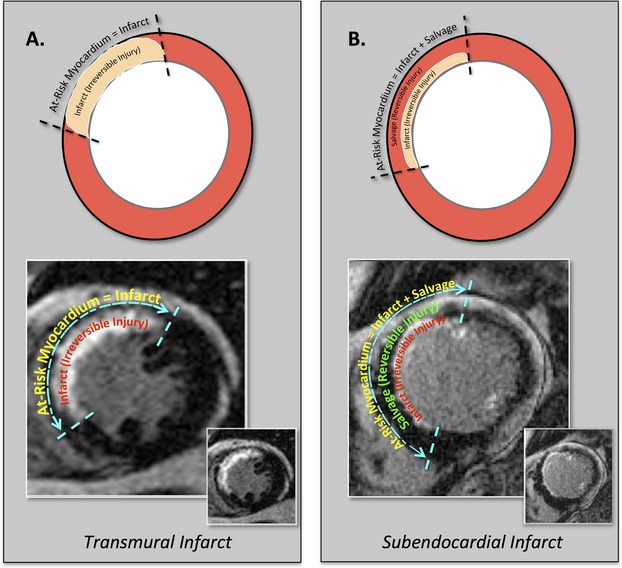
At‐risk myocardium=infarct (irreversible ischemic injury)+ salvage (reversible ischemic injury). Diagram establishing the relationships between at‐risk myocardium, infarct, and salvage in the setting of transmural and subendocardial myocardial infarction in the left anterior descending coronary artery territory.
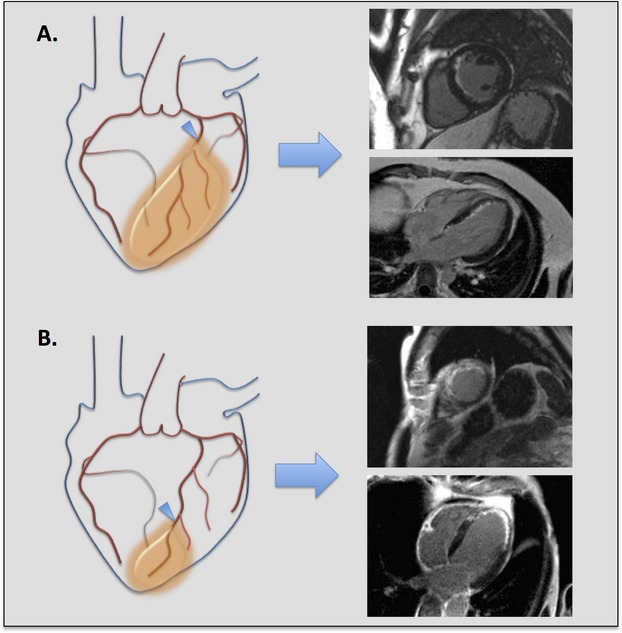
The importance of defining at‐risk myocardium, myocardial infarction, and myocardial salvage in the assessment of therapeutic efficacy for acute coronary syndrome. Two different examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory are illustrated. Corresponding delayed‐enhancement cardiac magnetic resonance (DE‐CMR) images in the short axis and 4 chamber orientations are shown for each example. Overall infarct size in each example is similar, but the amount of at‐risk myocardium and severity of ischemic injury differs. A, Proximal LAD occlusion (arrowhead) with large area of at‐risk myocardium (orange shading), subendocardial myocardial infarction, and significant myocardial salvage, suggesting less severe ischemic injury. B, Distal LAD occlusion (arrowhead) with small area of at‐risk myocardium (orange shading), transmural myocardial infarction, and no myocardial salvage, suggesting more severe ischemic injury.
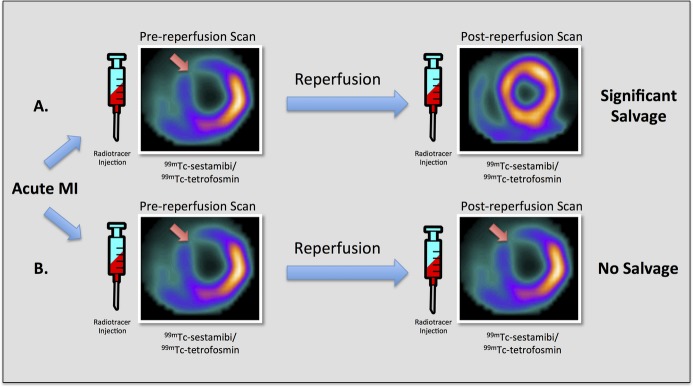
SPECT myocardial perfusion imaging for the assessment of at‐risk myocardium. Diagram depicting conventional technetium‐based SPECT myocardial perfusion imaging with 99mTc‐sestamibi/tetrofosmin for the assessment of myocardial salvage in 2 different hypothetical examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory. This technique requires 2 separate examinations with injection of radiotracer and imaging both before and after reperfusion. A, Pre‐reperfusion SPECT imaging reveals an area of decreased counts in the anteroseptum and anterior wall, whereas post‐reperfusion SPECT imaging shows normal myocardial perfusion. These findings suggest significant myocardial salvage in the left anterior descending coronary artery territory. B, Both pre‐reperfusion and postreperfusion SPECT images demonstrate decreased counts in the anteroseptum and anterior wall, suggesting no myocardial salvage in the left anterior descending coronary artery territory. 99mTc indicates technetium‐99m; MI, myocardial infarction; SPECT, single‐photon emission computed tomography.
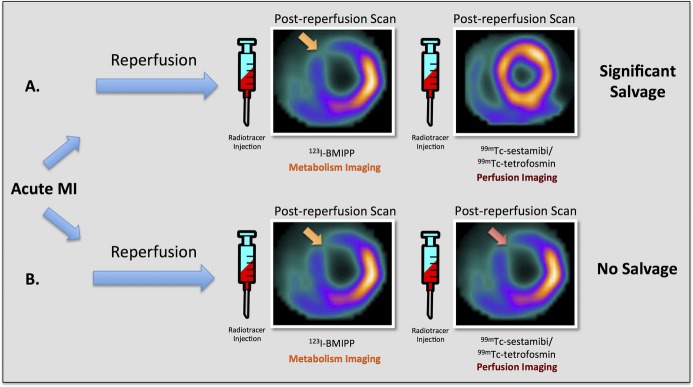
SPECT myocardial metabolism/perfusion imaging for the assessment of at‐risk myocardium. Diagram depicting combined fatty acid SPECT metabolic imaging with 123I‐BMIPP and technetium‐based SPECT perfusion imaging with 99mTc‐sestamibi/tetrofosmin for the assessment of myocardial salvage in 2 different hypothetical examples of acute ischemic myocardial injury in the left anterior descending (LAD) coronary artery territory. This technique requires injections of 2 separate radiotracers (123I‐BMIPP and 99mTc‐sestamibi/tetrofosmin) following reperfusion. A, Post‐reperfusion 123I‐BMIPP SPECT imaging reveals an area of decreased counts in the anteroseptum and anterior wall, whereas post‐reperfusion 99mTc‐sestamibi/tetrofosmin SPECT imaging shows normal myocardial perfusion. These findings suggest significant myocardial salvage in the left anterior descending coronary artery territory. B, Both post‐reperfusion 123I‐BMIPP SPECT metabolic imaging and post‐reperfusion 99mTc‐sestamibi/tetrofosmin perfusion SPECT imaging demonstrate decreased counts in the anteroseptum and anterior wall, suggesting no myocardial salvage in the left anterior descending coronary artery territory. 123I‐BMIPP indicates β‐methyl‐p‐[123I]‐iodophenyl‐pentadecanoic acid; 99mTc, technetium‐99m; MI, myocardial infarction; SPECT, single‐photon emission computed tomography.
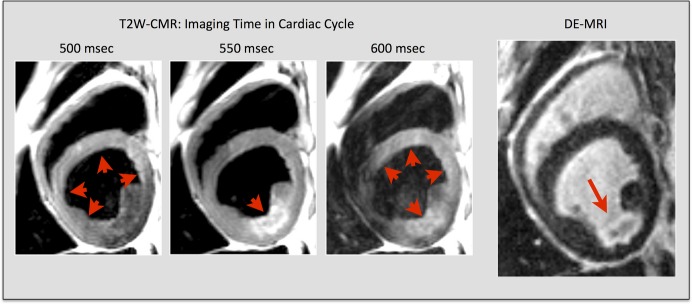
Technical issues with T2‐weighted CMR. Technical limitations with conventional dark‐blood T2W‐CMR. Images taken from a subject with myocardial infarction in the left circumflex coronary artery territory. Red arrowheads indicate areas of myocardium with high signal by T2W‐CMR. The red arrow indicates a subendocardial lateral wall infarct on corresponding DE‐CMR image at the same slice location. Note that the regional myocardial signal intensity varies significantly with small changes in the acquisition time of the cardiac cycle. (Adapted and reprinted, with permission, from reference no. .) DE‐CMR indicates delayed‐enhancement cardiac magnetic resonance; MRI, magnetic resonance imaging; T2W‐CMR, T2‐weighted cardiac magnetic resonance.
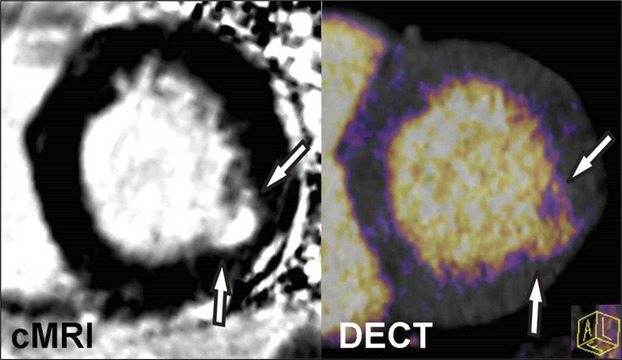
Cardiac magnetic resonance imaging (cMRI) and dual‐energy computed tomography (DECT) imaging of myocardial infarction. Iodine color map reconstructed from a DECT image demonstrates good agreement when compared with delayed‐enhancement cMRI of a subject with prior myocardial infarction of the lateral wall. Similar to cMRI, DECT offers the potential to assess myocardial infarction as well as myocardial salvage through the use of pre‐ and postcontrast techniques.
References
-
- Reimer KA, Jennings RB. The “wavefront phenomenon” of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979; 40:633-644 - PubMed
-
- Reimer KA, Lowe JE, Rasmussen MM, Jennings RB. The wavefront phenomenon of ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation. 1977; 56:786-794 - PubMed
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast‐enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000; 343:1445-1453 - PubMed
-
- Choi KM, Kim RJ, Gubernikoff G, Vargas JD, Parker M, Judd RM. Transmural extent of acute myocardial infarction predicts long‐term improvement in contractile function. Circulation. 2001; 104:1101-1107 - PubMed
-
- Burns RJ, Gibbons RJ, Yi Q, Roberts RS, Miller TD, Schaer GL, Anderson JL, Yusuf S. The relationships of left ventricular ejection fraction, end‐systolic volume index and infarct size to six‐month mortality after hospital discharge following myocardial infarction treated by thrombolysis. J Am Coll Cardiol. 2002; 39:30-36 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
