

Evaluation of American Joint Committee on Cancer, International Union Against Cancer, and Brigham and Women's Hospital tumor staging for cutaneous squamous cell carcinoma
- PMID: 24366933
- PMCID: PMC3897257
- DOI: 10.1200/JCO.2012.48.5326
Evaluation of American Joint Committee on Cancer, International Union Against Cancer, and Brigham and Women's Hospital tumor staging for cutaneous squamous cell carcinoma
Abstract
Purpose: To compare American Joint Committee on Cancer (AJCC), International Union Against Cancer (UICC), and Brigham and Women's Hospital (BWH) tumor (T) staging systems for cutaneous squamous cell carcinoma and validate BWH staging against prior data.
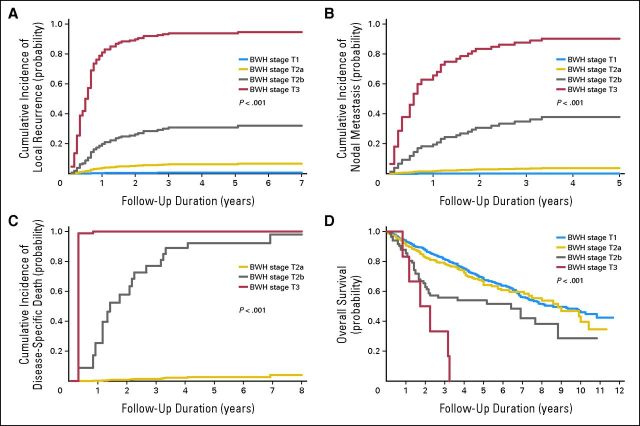
Patients and methods: Primary tumors diagnosed from 2000 to 2009 at BWH (n = 1,818) were analyzed. Poor outcomes (local recurrence [LR], nodal metastasis [NM], and disease-specific death [DSD]) were analyzed by T stage with regard to each staging system's distinctiveness (outcome differences between stages), homogeneity (outcome similarity within stages), and monotonicity (outcome worsening with increasing stage).
Results: AJCC and UICC T3 and T4 were indistinct with overlapping 95% CIs for 10-year cumulative incidences of poor outcomes, but all four BWH stages were distinct. AJCC and UICC high-stage tumors (T3/T4) were rare at 0.3% and 3% of the cohort, respectively. Most poor outcomes occurred in low stages (T1/T2; AJCC: 86% [95% CI, 77% to 91%]; UICC: 70% [61% to 79%]) resulting in heterogeneous outcomes in T1/T2. Conversely, in BWH staging, only 5% of tumors were high stage (T2b/T3), but they accounted for 60% (95% CI, 50% to 69%) of poor outcomes (70% of NMs and 83% of DSDs) indicating superior homogeneity and monotonicity as previously defined. Cumulative incidences of poor outcomes were low for BWH low-stage (T1/T2a) tumors (LR, 1.4% [95% CI, 1% to 2%]; NM, 0.6% [95% CI, 0% to 1%]; DSD, 0.2% [95% CI, 0% to 0.5%]) and higher for high-stage (T2b/T3) tumors (LR, 24% [95% CI, 16% to 34%]; NM, 24% [95% CI, 16% to 34%]; and DSD, 16% [95% CI, 10% to 25%], which validated an earlier study of an alternative staging system.
Conclusion: BWH staging offers improved distinctiveness, homogeneity, and monotonicity over AJCC and UICC staging. Population-based validation is needed. BWH T2b/T3 tumors define a high-risk group requiring further study for optimal management.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Skin cancer: Setting the stage for cutaneous SCC.Nat Rev Clin Oncol. 2014 Feb;11(2):63. doi: 10.1038/nrclinonc.2014.2. Epub 2014 Jan 21. Nat Rev Clin Oncol. 2014. PMID: 24445515 No abstract available.
References
-
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283–287. - PubMed
-
- Jambusaria-Pahlajani A, Miller CJ, Quon H, et al. Surgical monotherapy versus surgery plus adjuvant radiotherapy in high-risk cutaneous squamous cell carcinoma: A systematic review of outcomes. Dermatol Surg. 2009;35:574–585. - PubMed
-
- Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344:975–983. - PubMed
-
- Brantsch KD, Meisner C, Schönfisch B, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: A prospective study. Lancet Oncol. 2008;9:713–720. - PubMed
-
- Mourouzis C, Boynton A, Grant J, et al. Cutaneous head and neck SCCs and risk of nodal metastasis: UK experience. J Craniomaxillofac Surg. 2009;37:443–447. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
