

Stratification of risk of early-onset sepsis in newborns ≥ 34 weeks' gestation
- PMID: 24366992
- PMCID: PMC4079292
- DOI: 10.1542/peds.2013-1689
Stratification of risk of early-onset sepsis in newborns ≥ 34 weeks' gestation
Abstract
Objective: To define a quantitative stratification algorithm for the risk of early-onset sepsis (EOS) in newborns ≥ 34 weeks' gestation.
Methods: We conducted a retrospective nested case-control study that used split validation. Data collected on each infant included sepsis risk at birth based on objective maternal factors, demographics, specific clinical milestones, and vital signs during the first 24 hours after birth. Using a combination of recursive partitioning and logistic regression, we developed a risk classification scheme for EOS on the derivation dataset. This scheme was then applied to the validation dataset.
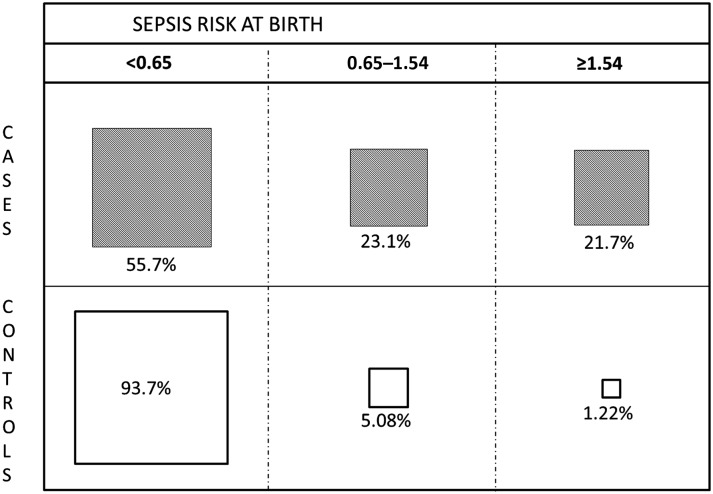
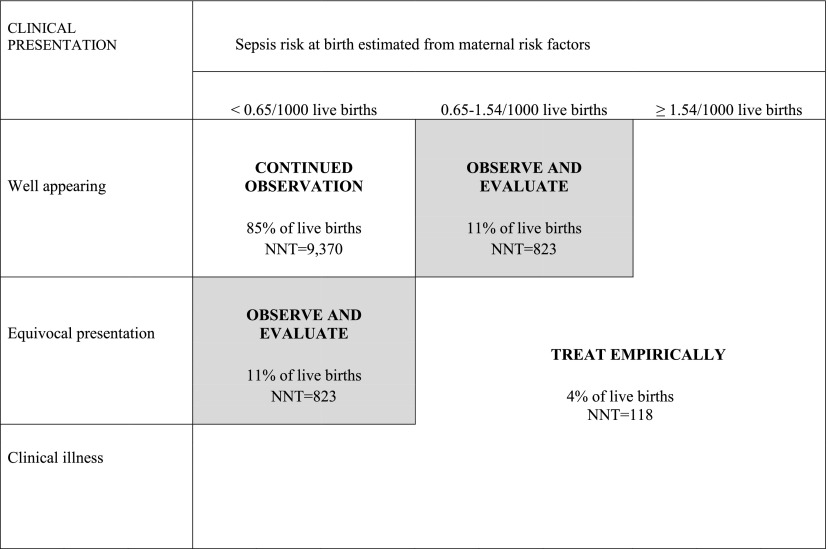
Results: Using a base population of 608,014 live births ≥ 34 weeks' gestation at 14 hospitals between 1993 and 2007, we identified all 350 EOS cases <72 hours of age and frequency matched them by hospital and year of birth to 1063 controls. Using maternal and neonatal data, we defined a risk stratification scheme that divided the neonatal population into 3 groups: treat empirically (4.1% of all live births, 60.8% of all EOS cases, sepsis incidence of 8.4/1000 live births), observe and evaluate (11.1% of births, 23.4% of cases, 1.2/1000), and continued observation (84.8% of births, 15.7% of cases, incidence 0.11/1000).
Conclusions: It is possible to combine objective maternal data with evolving objective neonatal clinical findings to define more efficient strategies for the evaluation and treatment of EOS in term and late preterm infants. Judicious application of our scheme could result in decreased antibiotic treatment in 80,000 to 240,000 US newborns each year.
Keywords: early-onset sepsis; late preterm infant; predictive modeling; term newborn.
Figures
Comment in
-
A data-based approach to evaluation and empiric treatment of newborn sepsis.J Pediatr. 2014 Sep;165(3):640-1. doi: 10.1016/j.jpeds.2014.06.033. J Pediatr. 2014. PMID: 25152158 No abstract available.
-
Reducing antibiotic use in asymptomatic term infants exposed to maternal chorioamnionitis: Predictive role of sepsis risk calculator.J Paediatr Child Health. 2022 Nov;58(11):1958-1963. doi: 10.1111/jpc.16128. Epub 2022 Jul 23. J Paediatr Child Health. 2022. PMID: 35869737
References
-
- Puopolo KM, Draper D, Wi S, et al. . Estimating the probability of neonatal early-onset infection on the basis of maternal risk factors. Pediatrics. 2011;128(5). Available at: www.pediatrics.org/cgi/content/full/128/5/e1155 - PMC - PubMed
-
- Schuchat A, Whitney C, Zangwill K, Centers for Disease Control and Prevention . Prevention of perinatal group B streptococcal disease: a public health perspective. MMWR Recomm Rep. 1996;45(RR-7):1–24 - PubMed
-
- Schuchat A, Zywicki SS, Dinsmoor MJ, et al. . Risk factors and opportunities for prevention of early-onset neonatal sepsis: a multicenter case-control study. Pediatrics. 2000;105(1 pt 1):21–26 - PubMed
-
- Bizzarro MJ, Raskind C, Baltimore RS, Gallagher PG. Seventy-five years of neonatal sepsis at Yale: 1928–2003. Pediatrics. 2005;116(3):595–602 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
