

Sonomammographic characteristics of invasive lobular carcinoma
- PMID: 24367199
- PMCID: PMC3846710
- DOI: 10.2147/BCTT.S34655
Sonomammographic characteristics of invasive lobular carcinoma
Abstract
Objective: The objective of our study was to identify characteristic features of invasive lobular carcinoma on mammography and ultrasound examinations.
Materials and methods: This is a retrospective multicenter study of women with biopsy-proven invasive lobular carcinoma. All patients had undergone diagnostic sonomammography. The imaging findings were identified by experienced breast imagers. Final surgical pathology results were used as the reference standard.
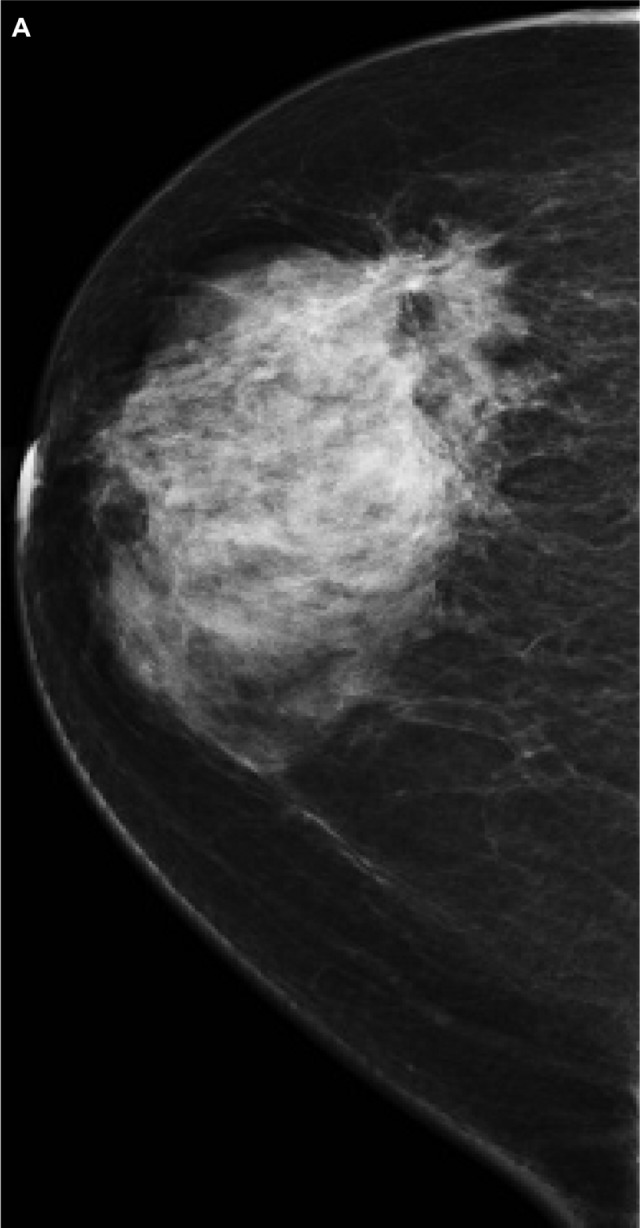
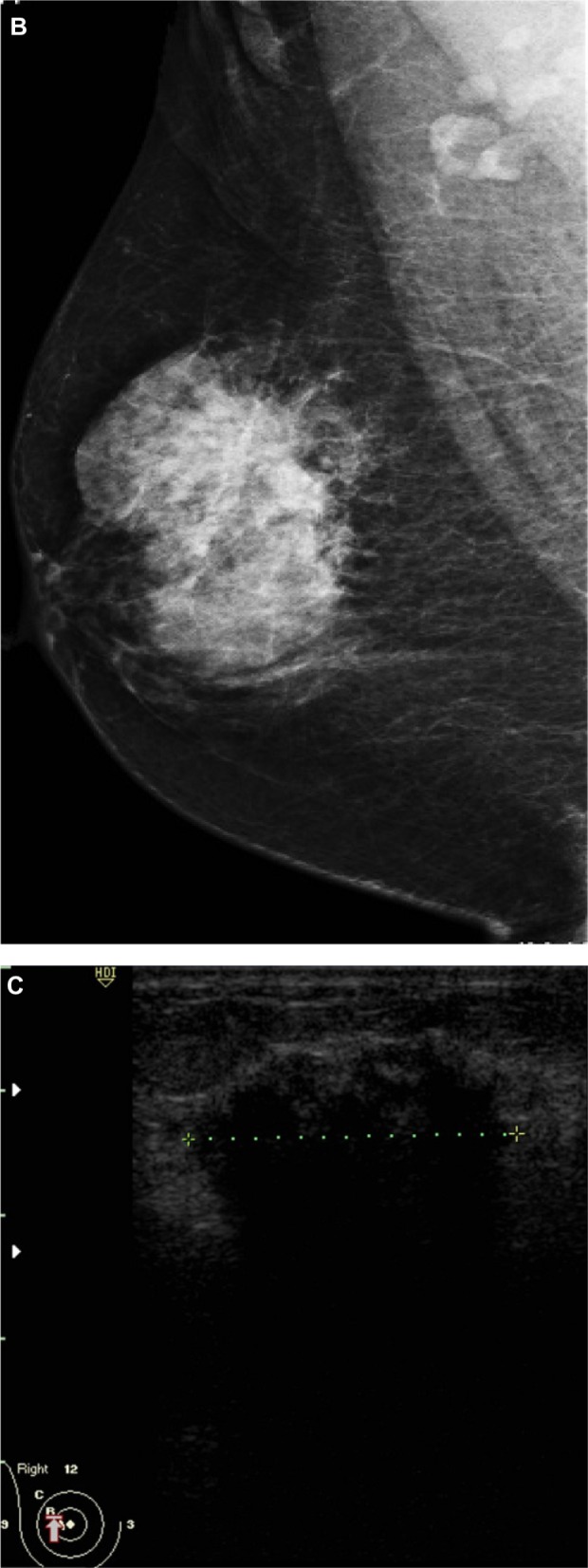
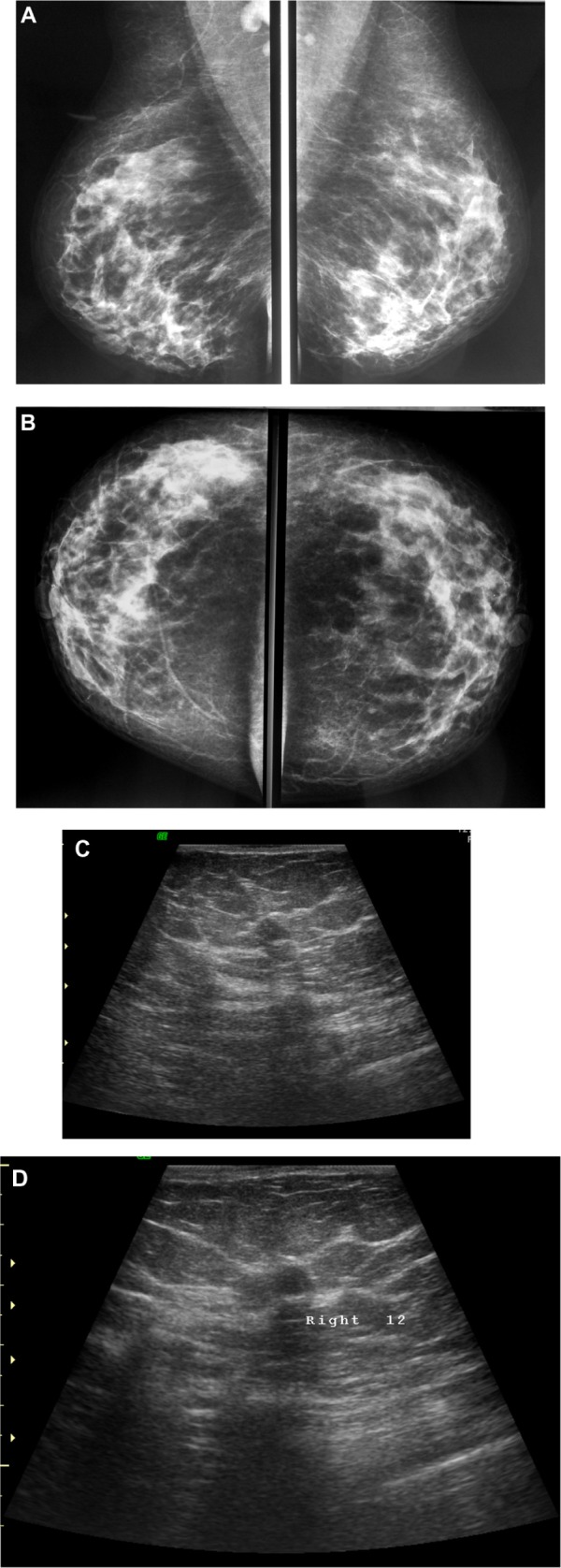
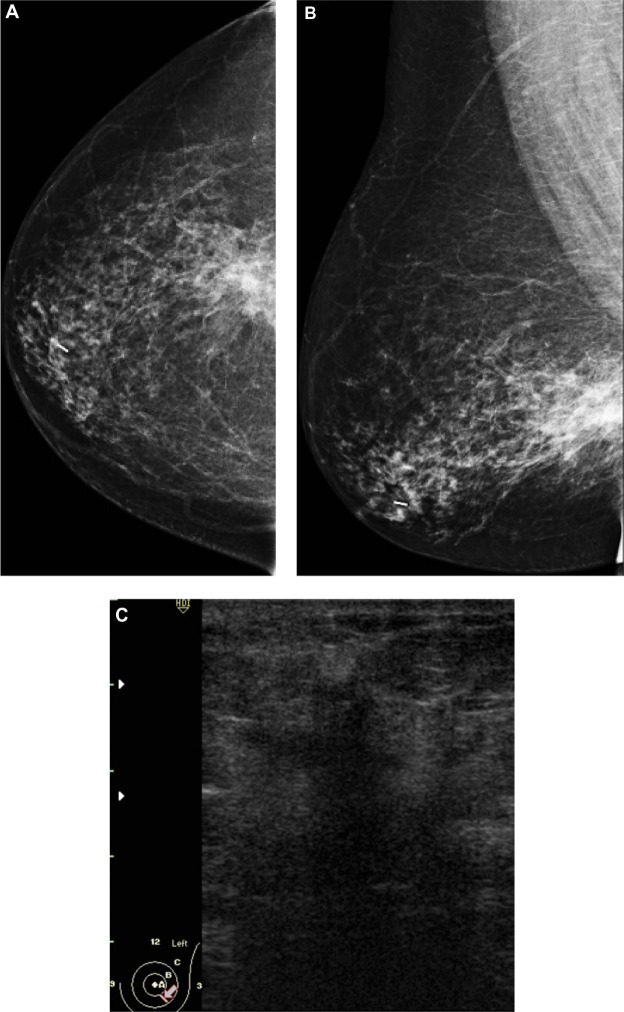
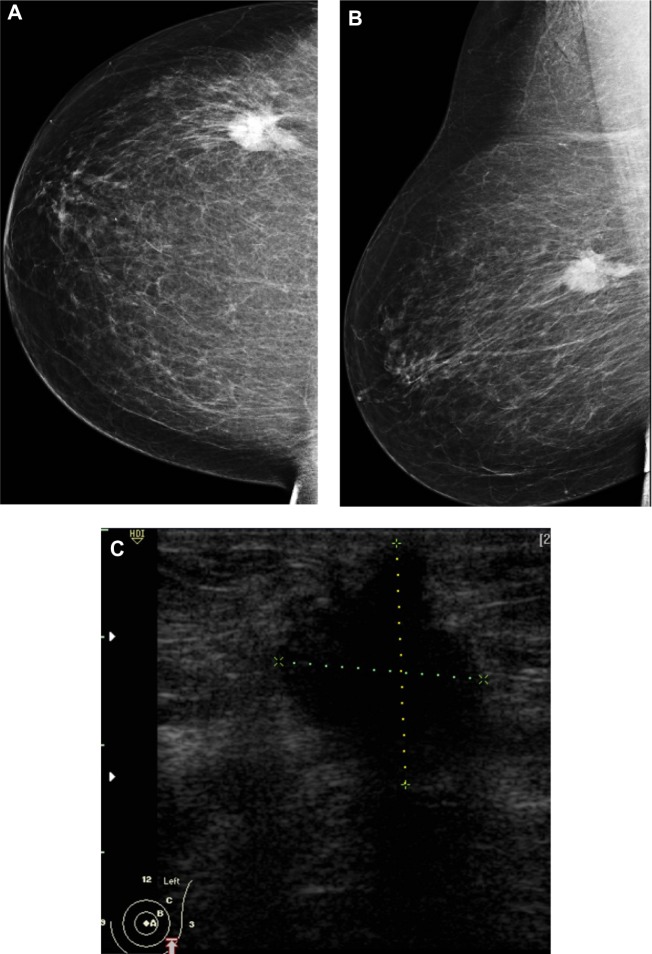
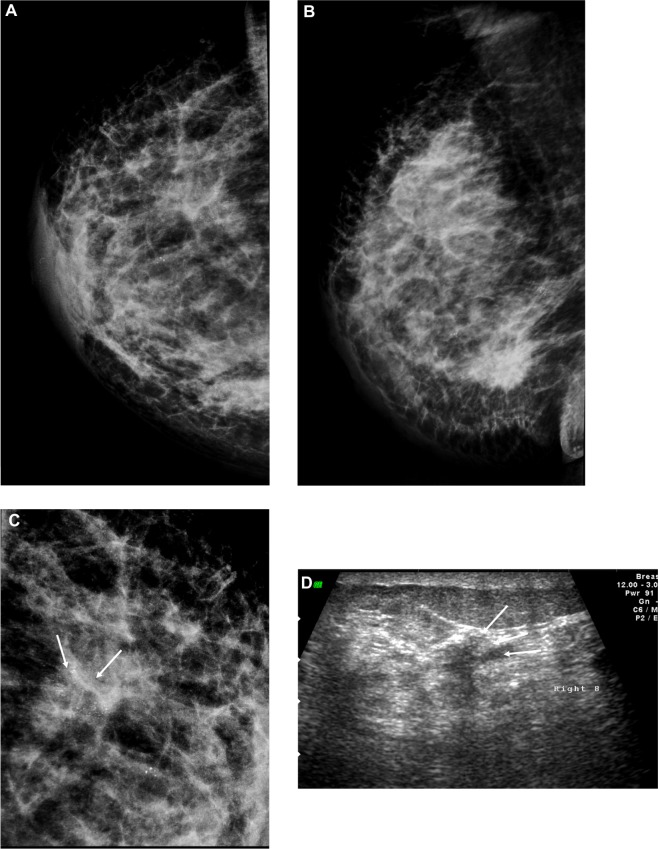
Results: Thirty-two women ranging in age from 42 to 63 years old (mean age, 53 years), All had biopsy-proven invasive lobular carcinomas. Common features on mammogram included dense mass followed by architectural distortion; three cases showed breast asymmetry and one case was reported as normal. On ultrasound, common features included solid mass with spiculated margins, posterior shadowing, and perpendicular to the skin.
Conclusion: Although no specific features could be linked to invasive lobular carcinoma, care should be directed to subtle signs such as architectural distortion and breast asymmetry in order not to miss any lesions. The combination of mammographic and sonographic helps to decrease the relatively high false negative diagnosis of this type of breast cancer.
Keywords: breast; cancer; mammography; ultrasound.
Figures
References
-
- Li CI, Daling JR. Changes in breast cancer incidence rates in the United States by histologic subtype and race/ethnicity, 1995 to 2004. Cancer Epidemiol Biomarkers Prev. 2007;16:2773–2780. - PubMed
-
- Kopans DB. Malignant lesions of the lobule. In: Kopans DB, editor. Breast Imaging. Baltimore, MD: Lippincott Williams & Wilkins; 2007. pp. 866–870.
-
- Rosenberg RD, Hunt WC, Williamson MR, et al. Effects of age, breast density, ethnicity, and estrogen replacement therapy on screening mammographic sensitivity and cancer stage at diagnosis: review of 183,134 screening mammograms in Albuquerque, New Mexico. Radiology. 1998;209:511–518. - PubMed
-
- Krecke KN, Gisvold JJ. Invasive lobular carcinoma of the breast: mammographic findings and extent of disease at diagnosis in 184 patients. AJR Am J Roentgenol. 1993;161:957–960. - PubMed
-
- Adejolu M, Krishnamurthy S, Whitman GJ. Ultrasound of invasive lobular carcinoma. Ultrasound Clin. 2011;6:313–325.
LinkOut - more resources
Full Text Sources
