

Optimal management of hepatorenal syndrome in patients with cirrhosis
- PMID: 24367209
- PMCID: PMC3846372
- DOI: 10.2147/hmer.s6918
Optimal management of hepatorenal syndrome in patients with cirrhosis
Abstract
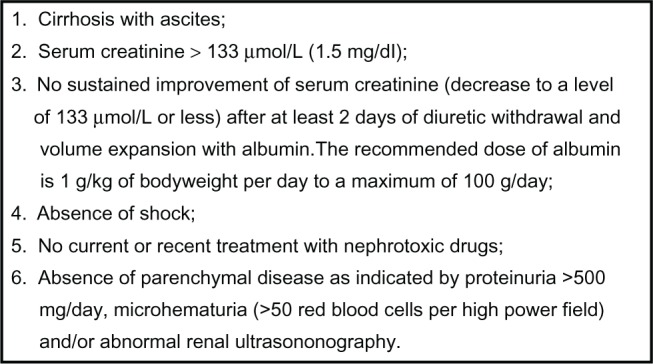
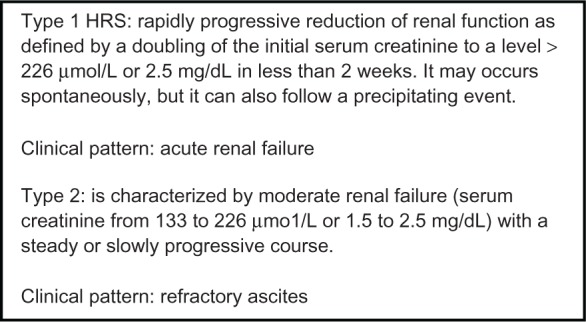
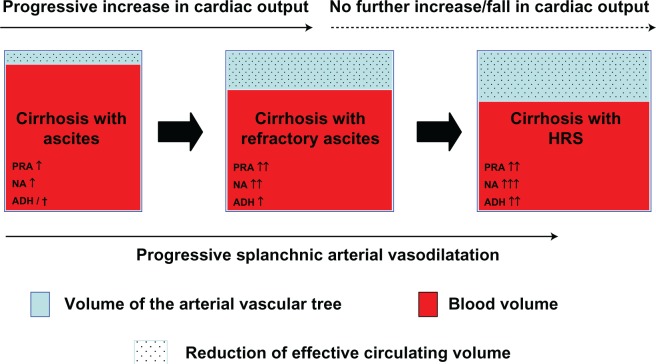
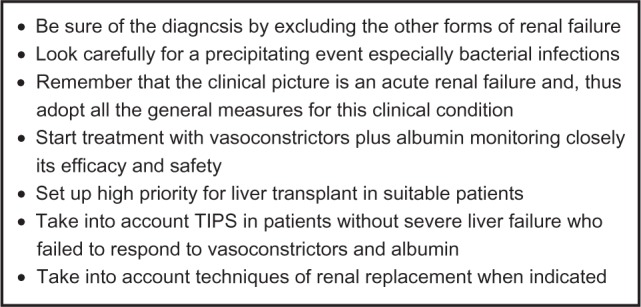
Hepatorenal syndrome (HRS) is a functional renal failure that often occurs in patients with cirrhosis and ascites. HRS develops as a consequence of a severe reduction of effective circulating volume due to both an extreme splanchnic arterial vasodilatation and a reduction of cardiac output. There are 2 different types of HRS. Type 1 HRS, which is often precipitated by a bacterial infection, especially spontaneous bacterial peritonitis, is characterized by a rapidly progressive impairment of renal function. Despite its functional origin, the prognosis of type 1 HRS is very poor. Type 2 HRS is characterized by a stable or slowly progressive renal failure so that its main clinical consequence is not acute renal failure but refractory ascites and its impact on prognosis is less negative. New treatments (vasoconstrictors plus albumin, transjugular portosystemic shunt, and molecular adsorbent recirculating system), which were introduced in the past 10 years, are effective in improving renal function in patients with HRS. Among these treatments vasoconstrictors plus albumin can also improve survival in patients with type 1 HRS. Thus, this therapeutic approach has changed the management of this severe complication in patients with advanced cirrhosis.
Keywords: acute renal injury; albumin; ascites; bacterial infections; chronic kidney disease; cirrhosis; midodrine; renal failure; renal replacement therapy; spontaneous bacterial peritonitis; terlipressin; transjugular portosystemic shunt; vasoconstrictors.
Figures
References
-
- Gines A, Escorsell A, Gines P, et al. Incidence, predictive factors and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology. 1993;105:229–236. - PubMed
-
- Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology. 1988;8:1151–1157. - PubMed
-
- Kanel GC, Peters RL. Glomerular tubular reflux – a morphologic renal lesion associated with the hepatorenal syndrome. Hepatology. 1984;4:242–246. - PubMed
-
- Arroyo V, Gines P, Gerbes AL, et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology. 1996;23:164–176. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
