

Moderate hyponatremia is associated with increased risk of mortality: evidence from a meta-analysis
- PMID: 24367479
- PMCID: PMC3867320
- DOI: 10.1371/journal.pone.0080451
Moderate hyponatremia is associated with increased risk of mortality: evidence from a meta-analysis
Abstract
Background: Hyponatremia is the most common electrolyte disorder in clinical practice, and evidence to date indicates that severe hyponatremia is associated with increased morbidity and mortality. The aim of our study was to perform a meta-analysis that included the published studies that compared mortality rates in subjects with or without hyponatremia of any degree.
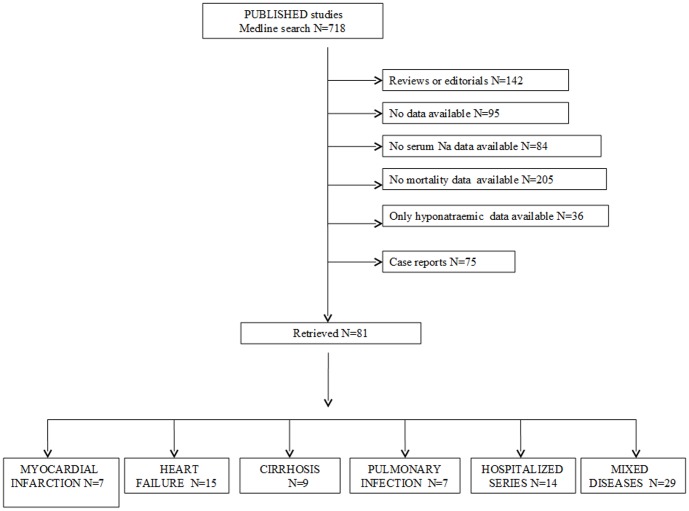
Methods and findings: An extensive Medline, Embase and Cochrane search was performed to retrieve the studies published up to October 1st 2012, using the following words: "hyponatremia" and "mortality". Eighty-one studies satisfied inclusion criteria encompassing a total of 850222 patients, of whom 17.4% were hyponatremic. The identification of relevant abstracts, the selection of studies and the subsequent data extraction were performed independently by two of the authors, and conflicts resolved by a third investigator. Across all 81 studies, hyponatremia was significantly associated with an increased risk of overall mortality (RR = 2.60[2.31-2.93]). Hyponatremia was also associated with an increased risk of mortality in patients with myocardial infarction (RR = 2.83[2.23-3.58]), heart failure (RR = 2.47[2.09-2.92]), cirrhosis (RR = 3.34[1.91-5.83]), pulmonary infections (RR = 2.49[1.44-4.30]), mixed diseases (RR = 2.59[1.97-3.40]), and in hospitalized patients (RR = 2.48[2.09-2.95]). A mean difference of serum [Na(+)] of 4.8 mmol/L was found in subjects who died compared to survivors (130.1 ± 5.6 vs 134.9 ± 5.1 mmol/L). A meta-regression analysis showed that the hyponatremia-related risk of overall mortality was inversely correlated with serum [Na(+)]. This association was confirmed in a multiple regression model after adjusting for age, gender, and diabetes mellitus as an associated morbidity.
Conclusions: This meta-analysis shows for the first time that even a moderate serum [Na(+)] decrease is associated with an increased risk of mortality in commonly observed clinical conditions across large numbers of patients.
Conflict of interest statement
Figures



References
-
- Upadhyay A, Jaber BL, Madias NE (2006) Incidence and prevalence of hyponatremia. Am J Med 119: 30–35. - PubMed
-
- Hoorn EJ, Lindemans J, Zietse R (2006) Development of severe hyponatremia in hospitalized patients: treatment-related risk factors and inadequate management. Nephrol Dial Transplant 28: 70–76. - PubMed
-
- Gill G, Huda B, Boyd A, Skagen K, Wile D, et al. (2006) Characteristics and mortality of severe hyponatremia – a hospital-based study. Clin Endocrinol (Oxf) 65: 246–249. - PubMed
-
- Adrogué HJ (2005) Consequences of inadequate management of hyponatremia. Am J Nephrol 25: 240–249. - PubMed
-
- Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G (2006) Mild chronic hyponatremia is associated with falls, unsteadiness and attention deficits. Am J Med 119: 71.e1–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
