

Incidence of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome and impact on patient outcome
- PMID: 24367678
- PMCID: PMC3867516
- DOI: 10.1371/journal.pone.0084585
Incidence of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome and impact on patient outcome
Erratum in
- PLoS One. 2014;9(1). doi:10.1371/annotation/15d01128-2495-4b95-8fe8-8702190fdb0e
Abstract
Objectives and design: We used data from a randomized trial of HIV-tuberculosis co-infected patients in Mozambique to determine the incidence and predictors of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome (IRIS) occurring within 12 weeks of starting antiretroviral therapy, and to evaluate its association with patient outcome at 48 weeks.
Methods: HIV-tuberculosis co-infected and antiretroviral therapy-naïve adults with less than 250 CD4/mm3 were randomized to a nevirapine or efavirenz-based antiretroviral therapy initiated 4 to 6 weeks after starting tuberculosis treatment, and were then followed for 48 weeks. Tuberculosis cases were diagnosed using WHO guidelines, and tuberculosis-IRIS by case definitions of the International Network for the Study of HIV-associated IRIS.
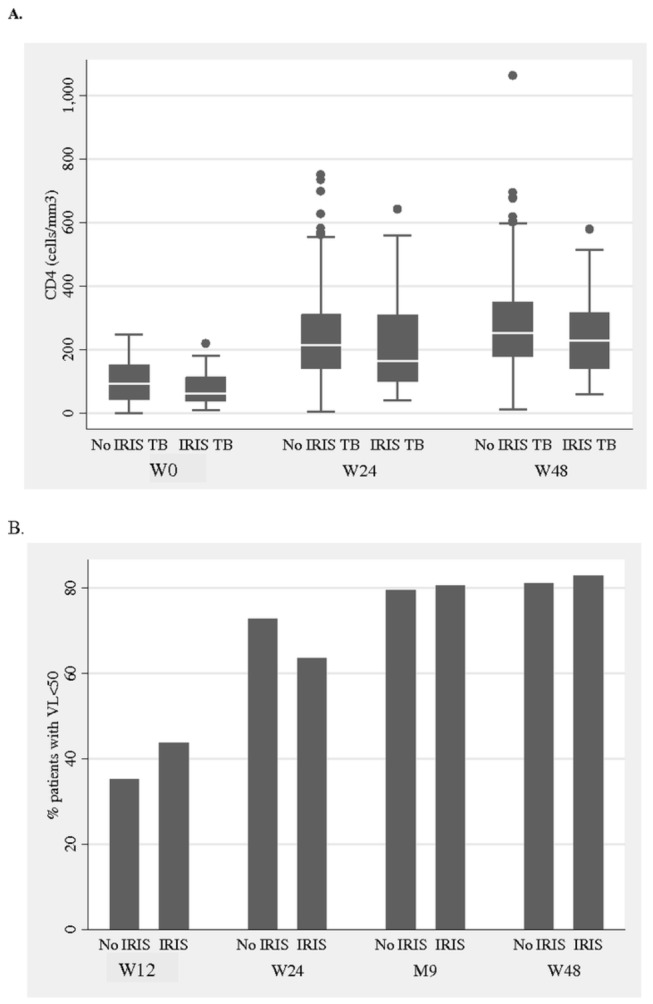
Results: The 573 HIV-tuberculosis co-infected patients who initiated antiretroviral therapy had a median CD4 count of 92 cells/mm(3) and HIV-1 RNA of 5.6 log10 copies/mL. Mortality at week 48 was 6.1% (35/573). Fifty-three (9.2%) patients presented a tuberculosis-IRIS within 12 weeks of starting antiretroviral therapy. Being female and having a low CD4 count, high HIV-1 RNA load, low body mass index and smear-positive pulmonary tuberculosis were independently associated with tuberculosis-IRIS. After adjustment for baseline body mass index, CD4 count and hemoglobin, occurrence of tuberculosis-IRIS was independently associated with 48-week mortality (aOR 2.72 95%CI 1.14-6.54). Immunological and HIV-1 virological responses and tuberculosis treatment outcomes were not different between patients with and without tuberculosis-IRIS.
Conclusion: In this large prospective cohort, tuberculosis-IRIS occurrence within 12 weeks of starting antiretroviral therapy was independently associated with the mortality of HIV-tuberculosis co-infected patients at 48 weeks post antiretroviral therapy initiation.
Conflict of interest statement
Figures


References
-
- Gupta A, Nadkarni G, Yang WT, Chandrasekhar A, Gupte N et al. (2011) Early mortality in adults initiating antiretroviral therapy (ART) in low- and middle-income countries (LMIC): a systematic review and meta-analysis. PLOS ONE 6: e28691. doi: 10.1371/journal.pone.0028691. PubMed: 22220193. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
