

A nonthoracotomy myocardial infarction model in an ovine using autologous platelets
- PMID: 24367790
- PMCID: PMC3866830
- DOI: 10.1155/2013/938047
A nonthoracotomy myocardial infarction model in an ovine using autologous platelets
Abstract
Objective: There is a paucity of a biological large animal model of myocardial infarction (MI). We hypothesized that, using autologous-aggregated platelets, we could create an ovine model that was reproducible and more closely mimicked the pathophysiology of MI.
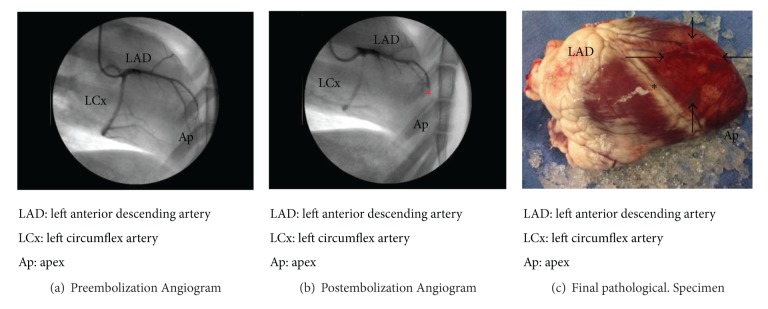
Methods: Mepacrine stained autologous platelets from male sheep (n = 7) were used to create a myocardial infarction via catheter injection into the mid-left anterior descending (LAD) coronary artery. Serial daily serum troponin measurements were taken and tissue harvested on post-embolization day three. Immunofluorescence microscopy was used to detect the mepacrine-stained platelet-induced thrombus, and histology performed to identify three distinct myocardial (infarct, peri-ischemic "border zone," and remote) zones.
Results: Serial serum troponin levels (μg/mL) measured 0.0 ± 0.0 at baseline and peaked at 297.4 ± 58.0 on post-embolization day 1, followed by 153.0 ± 38.8 on day 2 and 76.7 ± 19.8 on day 3. Staining confirmed distinct myocardial regions of inflammation and fibrosis as well as mepacrine-stained platelets as the cause of intravascular thrombosis.
Conclusion: We report a reproducible, unique model of a biological myocardial infarction in a large animal model. This technique can be used to study acute, regional myocardial changes following a thrombotic injury.
Figures



References
-
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) Journal of the American College of Cardiology. 2004;44(3):E1–E22. - PubMed
-
- Kwiatkowski P, Sai-Sudhakar C, Philips A, Parthasarathy S, Sun B. Development of a novel large animal model of ischemic heart failure using autologous platelet aggregates. International Journal of Artificial Organs. 2010;33(2):63–71. - PubMed
-
- Michael LH, Entman ML, Hartley CJ, et al. Myocardial ischemia and reperfusion: a murine model. American Journal of Physiology—Heart and Circulatory Physiology. 1995;269(6):H2147–H2154. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
