

Hospital volume and operative mortality in the modern era
- PMID: 24368634
- PMCID: PMC4069246
- DOI: 10.1097/SLA.0000000000000375
Hospital volume and operative mortality in the modern era
Abstract
Objective: To determine whether the relationship between hospital volume and mortality has changed over time.
Background: It is generally accepted that hospital volume is associated with mortality in high-risk procedures. However, as surgical safety has improved over the last decade, recent evidence has suggested that the inverse relationship has diminished or been eliminated.
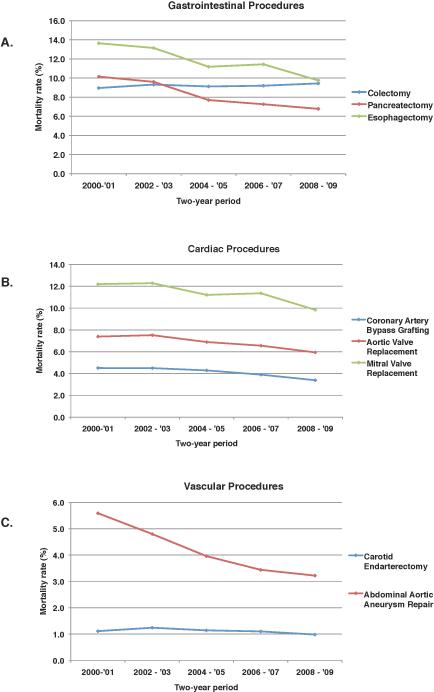
Methods: Using national Medicare claims data from 2000 through 2009, we examined mortality among 3,282,127 patients who underwent 1 of 8 gastrointestinal, cardiac, or vascular procedures. Hospitals were stratified into quintiles of operative volume. Using multivariable logistic regression models to adjust for patient characteristics, we examined the relationship between hospital volume and mortality, and assessed for changes over time. We performed sensitivity analyses using hierarchical logistic regression modeling with hospital-level random effects to confirm our results.
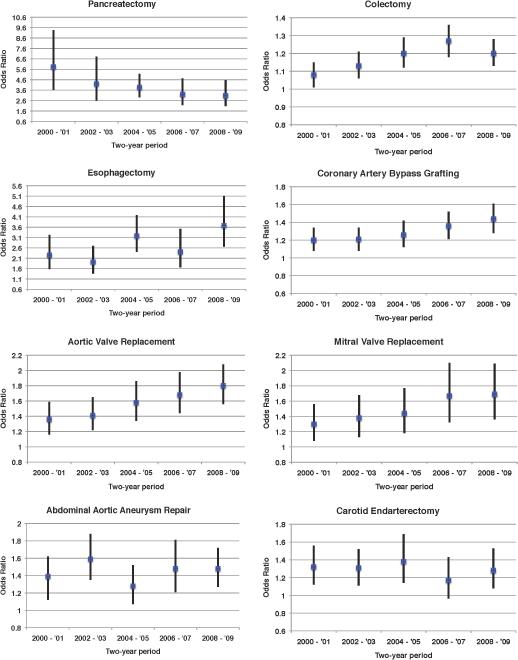
Results: Throughout the 10-year period, a significant inverse relationship was observed in all procedures. In 5 of the 8 procedures studied, the strength of the volume-outcome relationship increased over time. In esophagectomy, for example, the adjusted odds ratio of mortality in very low volume hospitals compared to very high volume hospitals increased from 2.25 [95% confidence interval (CI): 1.57-3.23] in 2000-2001 to 3.68 (95% CI: 2.66-5.11) in 2008-2009. Only pancreatectomy showed a notable decrease in strength of the relationship over time, from 5.83 (95% CI: 3.64-9.36) in 2000-2001, to 3.08 (95% CI: 2.07-4.57) in 2008-2009.
Conclusions: For all procedures examined, higher volume hospitals had significantly lower mortality rates than lower volume hospitals. Despite recent improvements in surgical safety, the strong inverse relationship between hospital volume and mortality persists in the modern era.
Figures
References
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–51. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–37. - PubMed
-
- Katz JN, Barrett J, Mahomed NN, et al. Association between hospital and surgeon procedure volume and the outcomes of total knee replacement. J Bone Joint Surg Am. 2004;86-A:1909–16. - PubMed
-
- Hannan EL, Kilburn H, Jr., O'Donnell JF, et al. Adult open heart surgery in New York State. An analysis of risk factors and hospital mortality rates. JAMA. 1990;264:2768–74. - PubMed
-
- Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007;356:486–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
