

Scapulothoracic anatomy and snapping scapula syndrome
- PMID: 24369502
- PMCID: PMC3863500
- DOI: 10.1155/2013/635628
Scapulothoracic anatomy and snapping scapula syndrome
Abstract
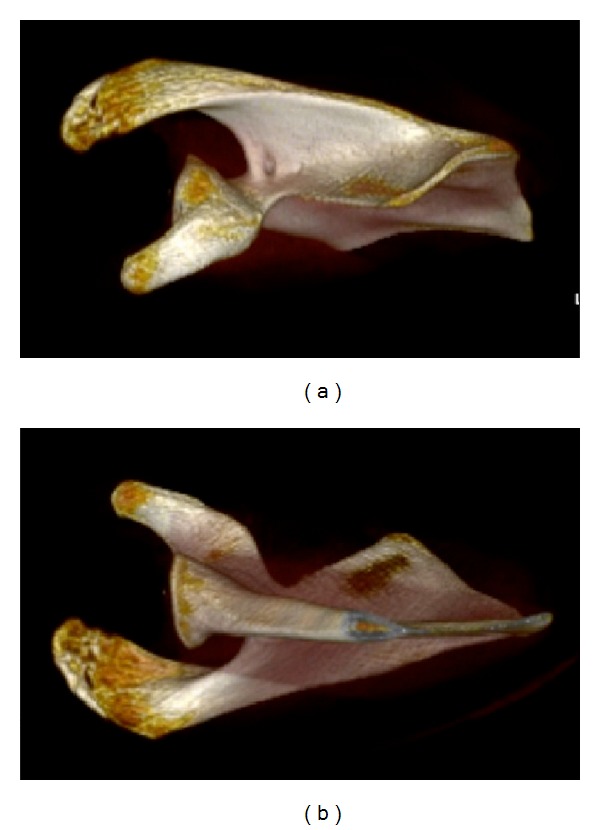
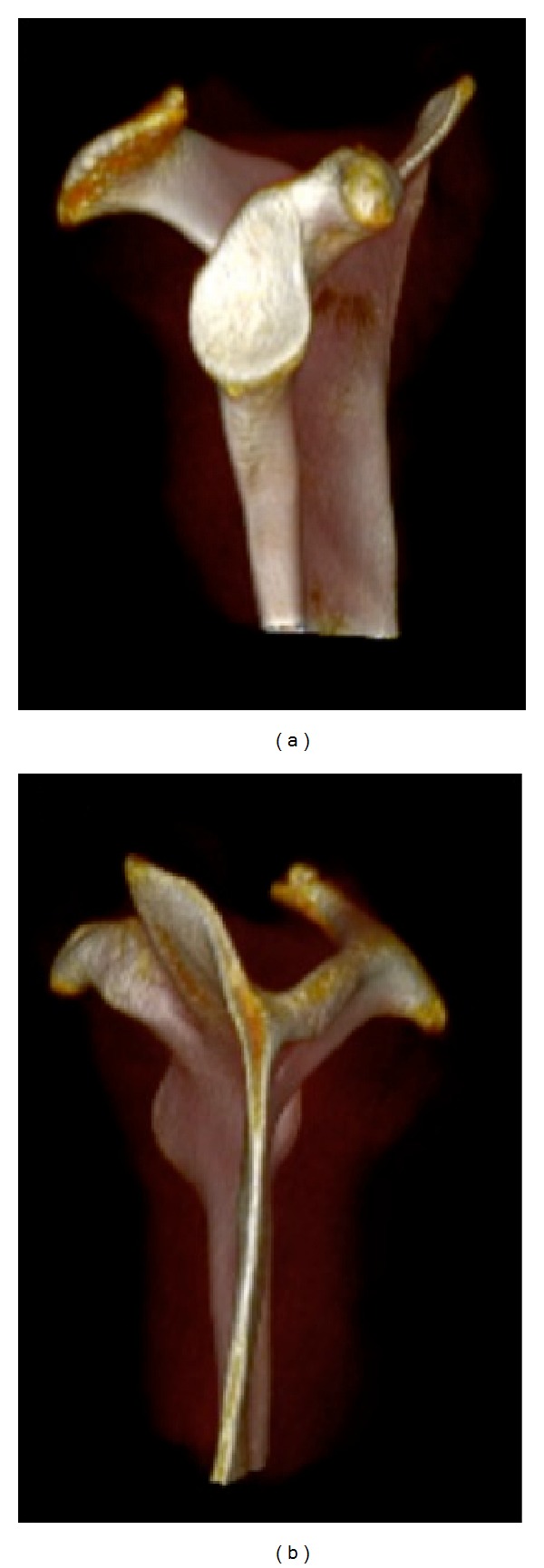
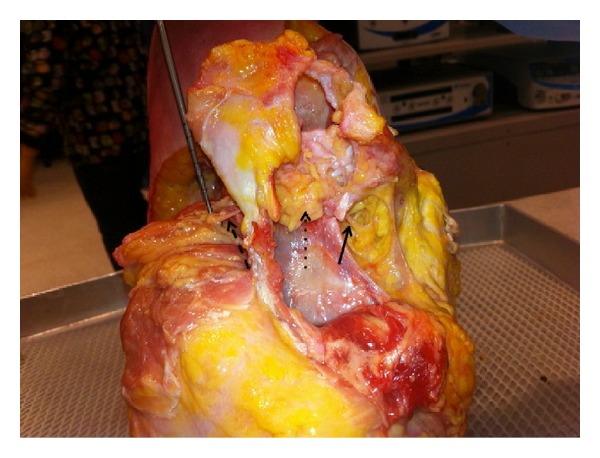
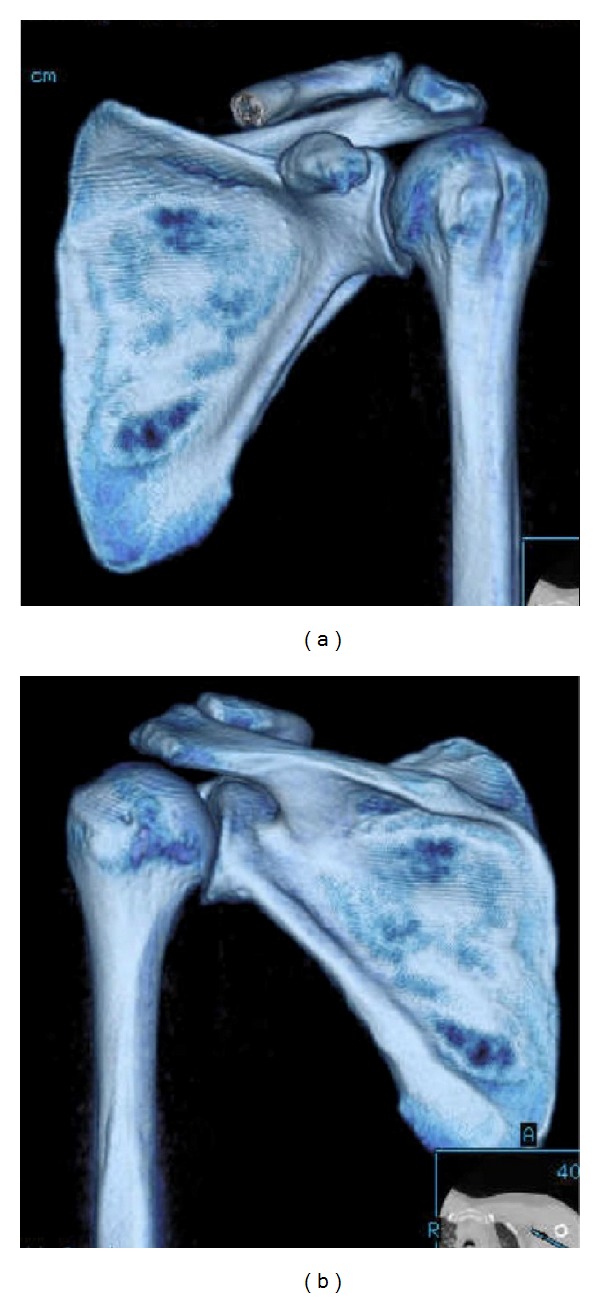
The scapulothoracic articulation is a sliding junction between the deep aspect of the scapula and thoracic rib cage at the levels of ribs 2 through 7. Motion at this articulation is dynamically stabilized by a variety of muscular attachments, allowing for controlled positioning of the glenoid to assist in glenohumeral joint function. A thorough understanding of the complex anatomic relationships, including the various muscles, and bursa, is critical to the evaluation of patients presenting with scapulothoracic disorders. The snapping scapula syndrome is caused by either osseous lesions or scapulothoracic bursitis and can be difficult to recognize and treat. The purpose of this review is to discuss the anatomy of the scapulothoracic articulation with an emphasis on the pathology associated with snapping scapula syndrome.
Figures


References
-
- Gaskill T, Millett PJ. Snapping scapula syndrome: diagnosis and management. Journal of the American Academy of Orthopaedic Surgeons. 2013;21(4):214–224. - PubMed
-
- Lazar MA, Kwon YW, Rokito AS. Snapping scapula syndrome. Journal of Bone and Joint Surgery A. 2009;91(9):2251–2262. - PubMed
-
- Mallon WJ, Brown HR, Vogler JB, III, Martinez S. Radiographic and geometric anatomy of the scapula. Clinical Orthopaedics and Related Research. 1992;(277):142–154. - PubMed
-
- Aggarwal A, Wahee P, Harjeet H, Aggarwal AK, Sahni D. Variable osseous anatomy of costal surface of scapula and its implications in relation to snapping scapula syndrome. Surgical and Radiologic Anatomy. 2011;33(2):135–140. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
