

Humeral shaft fracture treatment in the elite throwing athlete: a unique application of flexible intramedullary nailing
- PMID: 24369515
- PMCID: PMC3863509
- DOI: 10.1155/2013/546804
Humeral shaft fracture treatment in the elite throwing athlete: a unique application of flexible intramedullary nailing
Abstract
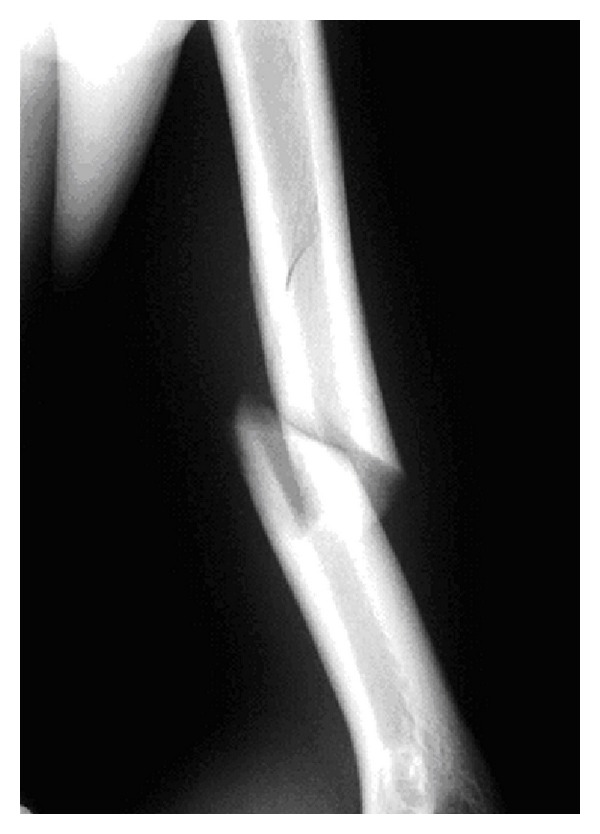
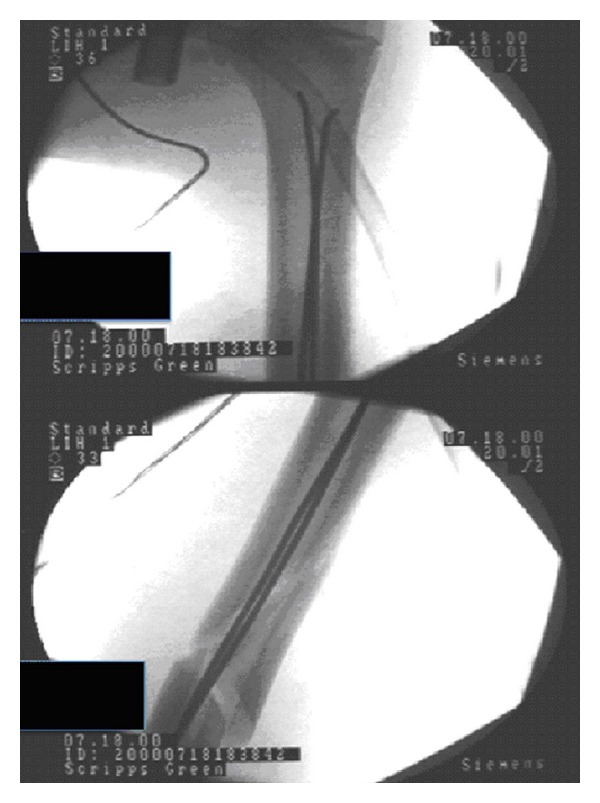
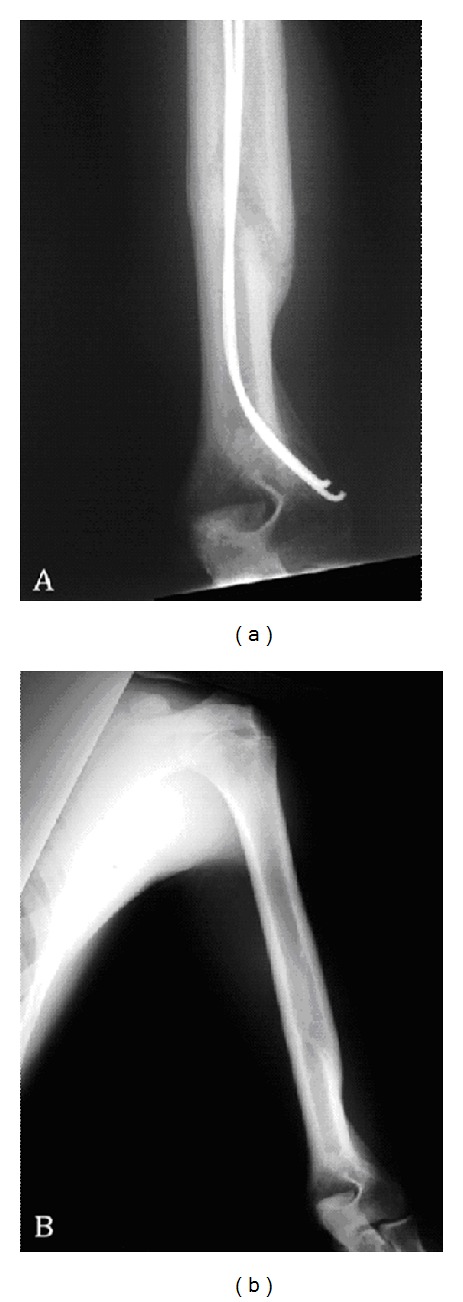
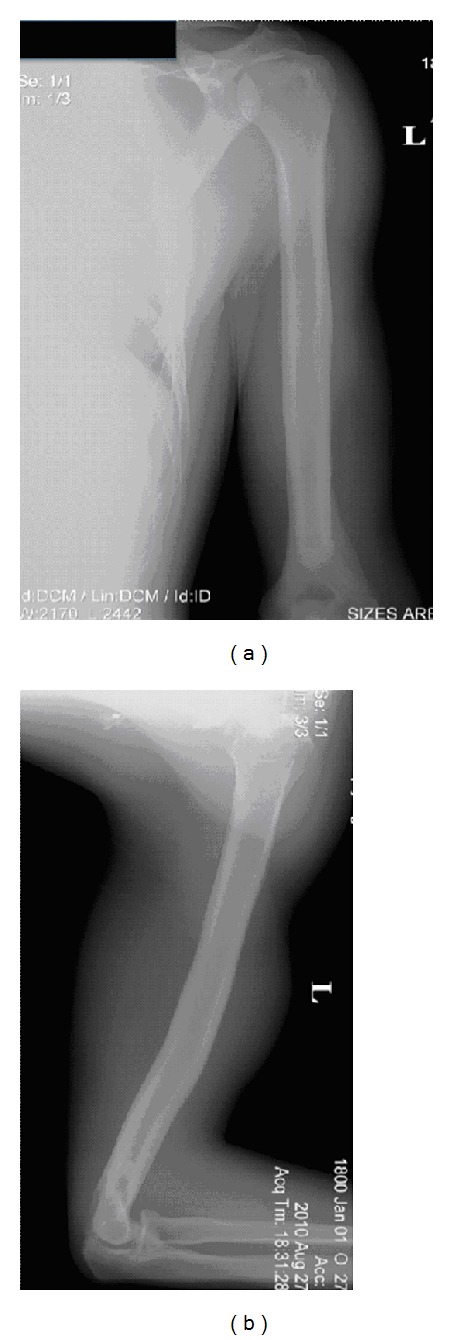
Humeral shaft stress fractures are being increasingly recognized as injuries that can significantly impact throwing mechanics if residual malalignment exists. While minimally displaced and angulated injuries are treated nonoperatively in a fracture brace, the management of significantly displaced humeral shaft fractures in the throwing athlete is less clear. Currently described techniques such as open reduction and internal fixation with plate osteosynthesis and rigid antegrade/retrograde locked intramedullary nailing have significant morbidity due to soft tissue dissection and damage. We present a case report of a high-level baseball pitcher whose significantly displaced humeral shaft stress fracture failed to be nonoperatively managed and was subsequently treated successfully with unlocked, retrograde flexible intramedullary nailing. The athlete was able to return to pitching baseball in one year and is currently pitching in Major League Baseball. We were able to recently collect 10-year follow-up data.
Figures
Similar articles
-
Shoulder function after surgical treatment of displaced fractures of the humeral shaft: a randomized trial comparing antegrade intramedullary nailing with minimally invasive plate osteosynthesis.J Shoulder Elbow Surg. 2014 Jun;23(6):767-74. doi: 10.1016/j.jse.2014.02.010. Epub 2014 Apr 24. J Shoulder Elbow Surg. 2014. PMID: 24768221 Clinical Trial.
-
[Antegrade and retrograde nailing of humeral shaft fractures].Oper Orthop Traumatol. 2021 Apr;33(2):139-159. doi: 10.1007/s00064-021-00706-x. Epub 2021 Apr 7. Oper Orthop Traumatol. 2021. PMID: 33825914 German.
-
Prospective randomized comparative study of antegrade and retrograde locked nailing for middle humeral shaft fracture.J Trauma. 2008 Jul;65(1):94-102. doi: 10.1097/TA.0b013e31812eed7f. J Trauma. 2008. PMID: 18580523 Clinical Trial.
-
Evidence-based update on the surgical treatment of pediatric tibial shaft fractures.Curr Opin Pediatr. 2019 Feb;31(1):92-102. doi: 10.1097/MOP.0000000000000704. Curr Opin Pediatr. 2019. PMID: 30461511 Review.
-
Management of humeral shaft fractures.J Am Acad Orthop Surg. 2012 Jul;20(7):423-33. doi: 10.5435/JAAOS-20-07-423. J Am Acad Orthop Surg. 2012. PMID: 22751161 Review.
Cited by
-
Surgical result of plate osteosynthesis using a locking plate system through an anterior humeral approach for distal shaft fracture of the humerus that occurred during a throwing motion.Int Orthop. 2016 Jul;40(7):1489-94. doi: 10.1007/s00264-015-2895-3. Epub 2015 Jul 23. Int Orthop. 2016. PMID: 26202018
References
-
- Branch T, Partin C, Chamberland P, Emeterio E, Sabetelle M. Spontaneous fractures of the humerus during pitching. A series of 12 cases. American Journal of Sports Medicine. 1992;20(4):468–470. - PubMed
-
- DiCicco JD, Mehlman CT, Urse JS. Fracture of the shaft of the humerus secondary to muscular violence. Journal of Orthopaedic Trauma. 1993;7(1):90–93. - PubMed
-
- Gore RM, Rogers LF, Bowerman J. Osseous manifestations of elbow stress associated with sports activities. American Journal of Roentgenology. 1980;134(5):971–977. - PubMed
-
- Hennigan SP, Bush-Joseph CA, Kuo KN, Bach BR., Jr. Throwing-induced humeral shaft fracture in skeletally immature adolescents. Orthopedics. 1999;22(6):621–622. - PubMed
-
- Kuschner SH, Lane CS. Recurrent fracture of the humerus in a softball player. American Journal of Orthopedics. 1999;28(11):654–656. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
