

Impact of DECISION + 2 on patient and physician assessment of shared decision making implementation in the context of antibiotics use for acute respiratory infections
- PMID: 24369771
- PMCID: PMC3879432
- DOI: 10.1186/1748-5908-8-144
Impact of DECISION + 2 on patient and physician assessment of shared decision making implementation in the context of antibiotics use for acute respiratory infections
Abstract
Background: DECISION + 2, a training program for physicians, is designed to implement shared decision making (SDM) in the context of antibiotics use for acute respiratory tract infections (ARTIs). We evaluated the impact of DECISION + 2 on SDM implementation as assessed by patients and physicians, and on physicians' intention to engage in SDM.
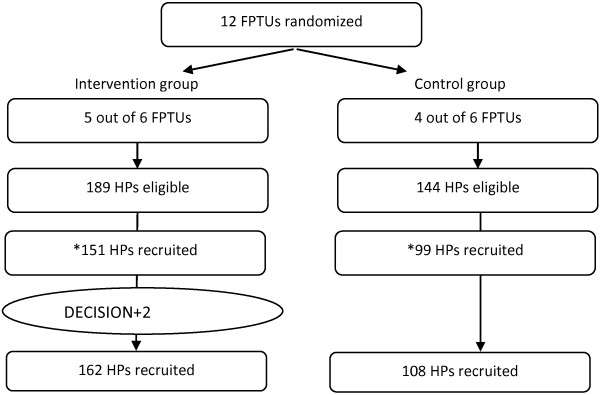
Methods: From 2010 to 2011, a multi-center, two-arm, parallel randomized clustered trial appraised the effects of DECISION + 2 on the decision to use antibiotics for patients consulting for ARTIs. We randomized 12 family practice teaching units (FPTUs) to either DECISION + 2 or usual care. After the consultation, both physicians and patients independently completed questionnaires based on the D-Option scale regarding SDM behaviors during the consultation. Patients also answered items assessing the role they assumed during the consultation (active/collaborative/passive). Before and after the intervention, physicians completed a questionnaire based on the Theory of Planned Behavior to measure their intention to engage in SDM. To account for the cluster design, we used generalized estimating equations and generalized linear mixed models to assess the impact of DECISION + 2 on the outcomes of interest.
Results: A total of 270 physicians (66% women) participated in the study. After DECISION + 2, patients' D-Option scores were 80.1 ± 1.1 out of 100 in the intervention group and 74.9 ± 1.1 in the control group (p = 0.001). Physicians' D-Option scores were 79.7 ± 1.8 in the intervention group and 76.3 ± 1.9 in the control group (p = 0.2). However, subgroup analyses showed that teacher physicians D-Option scores were 79.7 ± 1.5 and 73.0 ± 1.4 respectively (p = 0.001). More patients reported assuming an active or collaborative role in the intervention group (67.1%), than in the control group (49.2%) (p = 0.04). There was a significant relation between patients' and physicians' D-Option scores (p < 0.01) and also between patient-reported assumed roles and both D-Option scores (as assessed by patients, p < 0.01; and physicians, p = 0.01). DECISION + 2 had no impact on the intention of physicians to engage in SDM.
Conclusion: DECISION + 2 positively influenced SDM behaviors as assessed by patients and teacher physicians. Physicians' intention to engage in SDM was not affected by DECISION + 2.
Trial registration: ClinicalTrials.gov trials register no. NCT01116076.
Figures

References
-
- Butler CC, Hood K, Verheij T, Little P, Melbye H, Nuttall J, Kelly MJ, Molstad S, Godycki-Cwirko M, Almirall J. et al.Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: prospective study in 13 countries. BMJ. 2009;8:b2242. doi: 10.1136/bmj.b2242. - DOI - PMC - PubMed
-
- Legare F, Labrecque M, Godin G, LeBlanc A, Laurier C, Grimshaw J, Castel J, Tremblay I, Fremont P, Cauchon M. et al.Training family physicians and residents in family medicine in shared decision making to improve clinical decisions regarding the use of antibiotics for acute respiratory infections: protocol for a clustered randomized controlled trial. BMC Fam Pract. 2011;8:3. doi: 10.1186/1471-2296-12-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
