

Pharmacogenetics: implications of race and ethnicity on defining genetic profiles for personalized medicine
- PMID: 24369795
- PMCID: PMC3933289
- DOI: 10.1016/j.jaci.2013.10.040
Pharmacogenetics: implications of race and ethnicity on defining genetic profiles for personalized medicine
Abstract
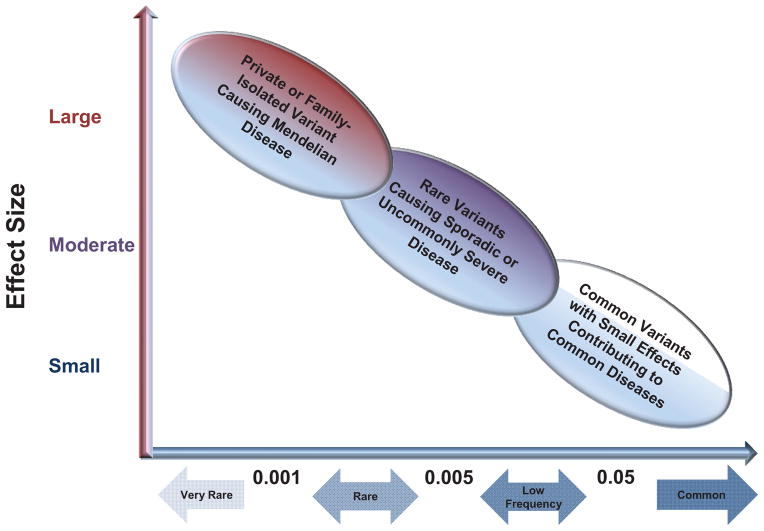
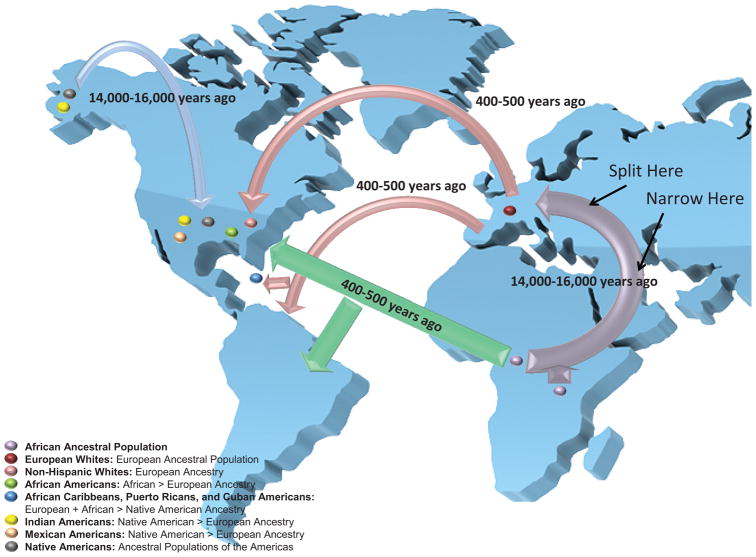
Pharmacogenetics is being used to develop personalized therapies specific to subjects from different ethnic or racial groups. To date, pharmacogenetic studies have been primarily performed in trial cohorts consisting of non-Hispanic white subjects of European descent. A "bottleneck" or collapse of genetic diversity associated with the first human colonization of Europe during the Upper Paleolithic period, followed by the recent mixing of African, European, and Native American ancestries, has resulted in different ethnic groups with varying degrees of genetic diversity. Differences in genetic ancestry might introduce genetic variation, which has the potential to alter the therapeutic efficacy of commonly used asthma therapies, such as β2-adrenergic receptor agonists (β-agonists). Pharmacogenetic studies of admixed ethnic groups have been limited to small candidate gene association studies, of which the best example is the gene coding for the receptor target of β-agonist therapy, the β2-adrenergic receptor (ADRB2). Large consortium-based sequencing studies are using next-generation whole-genome sequencing to provide a diverse genome map of different admixed populations, which can be used for future pharmacogenetic studies. These studies will include candidate gene studies, genome-wide association studies, and whole-genome admixture-based approaches that account for ancestral genetic structure, complex haplotypes, gene-gene interactions, and rare variants to detect and replicate novel pharmacogenetic loci.
Keywords: ADRB1; ADRB2; Asthma; BADGER; BARGE; Best Add-on Therapy Giving Effective Response Trial; Beta Agonist Response by Genotype Trial; CAAPA; Consortium on Asthma among African-ancestry Populations in the Americas; G protein receptor kinase 5; GALA; GLCCl1; GRK5; GWAS; Genetics of Asthma in Latino Americans; Genome-wide association study; Glucocorticoid-induced transcript 1 gene; ICS; Inhaled corticosteroid; LABA; LARGE; Long-acting Beta Agonist Response by Genotype; Long-acting β-agonist; NHLBI; NIH; National Heart, Lung, and Blood Institute; National Institutes of Health; PEFR; Peak expiratory flow rate; SABA; SMART; SNP; SPATS2L; Salmeterol Multicenter Asthma Research Trial; Short-acting β-agonist; Single nucleotide polymorphism; Spermatogenesis-associated, serine-rich 2-like gene; admixture mapping; ethnic group; genes; pharmacogenetics; response heterogeneity; single nucleotide polymorphism; β(1)-Adrenergic receptor; β(2)-Adrenergic receptor.
Copyright © 2013 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Dries DL, Exner DV, Gersh BJ, Cooper HA, Carson PE, Domanski MJ. Racial differences in the outcome of left ventricular dysfunction. New Engl J Med. 1999;340(8):609–16. - PubMed
-
- Beta-Blocker Evaluation of Survival Trial I. A trial of the beta-blocker bucindolol in patients with advanced chronic heart failure. New Engl J Med. 2001;344(22):1659–67. - PubMed
-
- Vesell ES. Pharmacogenetic perspectives gained from twin and family studies. Pharmacol Ther. 1989;41(3):535–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
