

Renal relevant radiology: radiologic imaging in autosomal dominant polycystic kidney disease
- PMID: 24370765
- PMCID: PMC3913246
- DOI: 10.2215/CJN.08940813
Renal relevant radiology: radiologic imaging in autosomal dominant polycystic kidney disease
Abstract
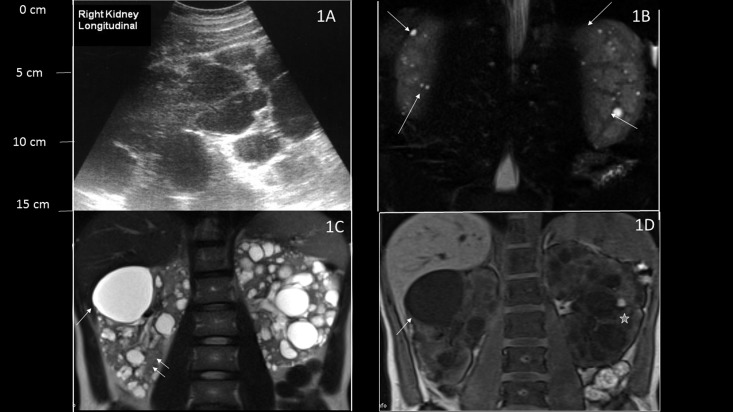
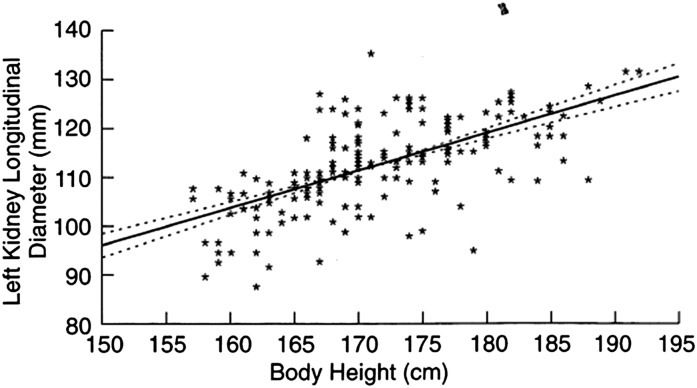
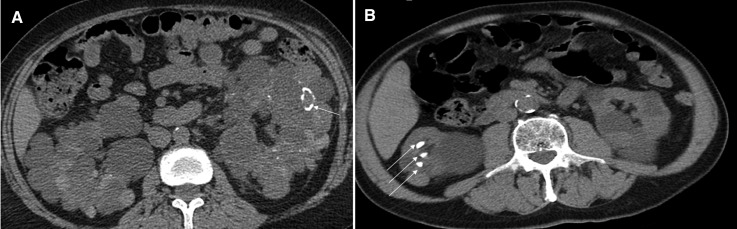
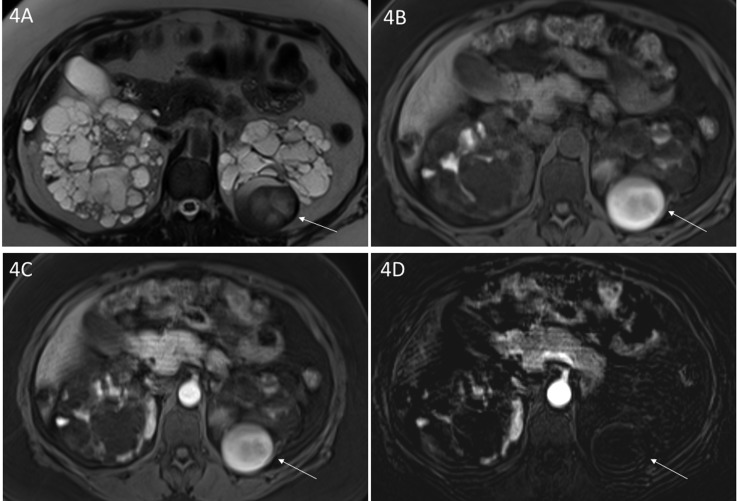
Autosomal-dominant polycystic kidney disease is a systemic disorder and the most common hereditary renal disease, which is characterized by cyst growth, progressive renal enlargement, and development of renal failure. The cystic nature of autosomal dominant polycystic kidney disease and its renal and extrarenal complications (kidney stones, cyst hemorrhage, intracerebral aneurysm, liver cysts, cardiac valve abnormalities, etc.) give radiologic imaging studies a central role in the management of these patients. This article reviews the indications, comparative use, and limitation of various imaging modalities (ultrasonography, magnetic resonance imaging, computerized tomography scan, Positron emission tomography scan, and renal scintigraphy) for the diagnosis and management of complications in autosomal dominant polycystic kidney disease. Finally, this work provides evidence for the value of total kidney volume to predict disease progression in autosomal dominant polycystic kidney disease.
Figures
Similar articles
-
A Review of the Imaging Techniques for Measuring Kidney and Cyst Volume in Establishing Autosomal Dominant Polycystic Kidney Disease Progression.Am J Nephrol. 2018;48(1):67-78. doi: 10.1159/000491022. Epub 2018 Aug 2. Am J Nephrol. 2018. PMID: 30071518 Review.
-
[Renal failure and cystic kidney diseases].J Radiol. 2011 Apr;92(4):308-22. doi: 10.1016/j.jradio.2011.02.021. Epub 2011 Apr 21. J Radiol. 2011. PMID: 21549887 Review. French.
-
Diagnostic approach in autosomal dominant polycystic kidney disease.Clin J Am Soc Nephrol. 2006 Sep;1(5):1108-14. doi: 10.2215/CJN.02190606. Epub 2006 Aug 9. Clin J Am Soc Nephrol. 2006. PMID: 17699332 Review.
-
Segmentation of individual renal cysts from MR images in patients with autosomal dominant polycystic kidney disease.Clin J Am Soc Nephrol. 2013 Jul;8(7):1089-97. doi: 10.2215/CJN.10561012. Epub 2013 Mar 21. Clin J Am Soc Nephrol. 2013. PMID: 23520042 Free PMC article.
-
Renal structure in early autosomal-dominant polycystic kidney disease (ADPKD): The Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) cohort.Kidney Int. 2003 Sep;64(3):1035-45. doi: 10.1046/j.1523-1755.2003.00185.x. Kidney Int. 2003. PMID: 12911554
Cited by
-
Pravastatin Therapy and Biomarker Changes in Children and Young Adults with Autosomal Dominant Polycystic Kidney Disease.Clin J Am Soc Nephrol. 2015 Sep 4;10(9):1534-41. doi: 10.2215/CJN.11331114. Epub 2015 Jul 29. Clin J Am Soc Nephrol. 2015. PMID: 26224879 Free PMC article. Clinical Trial.
-
Cystic Kidney Diseases That Require a Differential Diagnosis from Autosomal Dominant Polycystic Kidney Disease (ADPKD).J Clin Med. 2022 Nov 3;11(21):6528. doi: 10.3390/jcm11216528. J Clin Med. 2022. PMID: 36362756 Free PMC article. Review.
-
Conventional uroradiology with excretory urography: a forgotten art?Br J Radiol. 2022 Apr 1;95(1132):20210949. doi: 10.1259/bjr.20210949. Epub 2022 Jan 7. Br J Radiol. 2022. PMID: 34990261 Free PMC article. Review.
-
How simple are 'simple renal cysts'?Nephrol Dial Transplant. 2014 Sep;29 Suppl 4(Suppl 4):iv106-12. doi: 10.1093/ndt/gfu106. Nephrol Dial Transplant. 2014. PMID: 25165175 Free PMC article. Review.
-
The spectrum of autosomal dominant polycystic kidney disease in children and adolescents.Pediatr Nephrol. 2017 Jan;32(1):31-42. doi: 10.1007/s00467-016-3364-y. Epub 2016 Mar 31. Pediatr Nephrol. 2017. PMID: 27034070 Review.
References
-
- Gabow PA: Autosomal dominant polycystic kidney disease. N Engl J Med 329: 332–342, 1993 - PubMed
-
- Hateboer N, v Dijk MA, Bogdanova N, Coto E, Saggar-Malik AK, San Millan JL, Torra R, Breuning M, Ravine D: Comparison of phenotypes of polycystic kidney disease types 1 and 2. European PKD1-PKD2 Study Group. Lancet 353: 103–107, 1999 - PubMed
-
- Rahbari-Oskoui F, Taylor AP, O'Neill WC: Ultrasonography and nuclear medicine. In: Schrier's Diseases of the Kidney, Vol. 1, 9th Ed., edited by Schrier RW, Philadelphia, Lippincott Williams & Wilkins, 2012
-
- Reed B, Nobakht E, Dadgar S, Bekheirnia MR, Masoumi A, Belibi F, Yan XD, Cadnapaphornchai M, Schrier RW: Renal ultrasonographic evaluation in children at risk of autosomal dominant polycystic kidney disease. Am J Kidney Dis 56: 50–56, 2010 - PubMed
-
- Levine E, Hartman DS, Meilstrup JW, Van Slyke MA, Edgar KA, Barth JC: Current concepts and controversies in imaging of renal cystic diseases. Urol Clin North Am 24: 523–543, 1997 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
