

Buttonhole cannulation and clinical outcomes in a home hemodialysis cohort and systematic review
- PMID: 24370768
- PMCID: PMC3878698
- DOI: 10.2215/CJN.03930413
Buttonhole cannulation and clinical outcomes in a home hemodialysis cohort and systematic review
Abstract
Background and objectives: The relative merits of buttonhole (or blunt needle) versus rope ladder (or sharp needle) cannulation for hemodialysis vascular access are unclear.
Design, setting, participants, & measurements: Clinical outcomes by cannulation method were reviewed in 90 consecutive home hemodialysis patients. Initially, patients were trained in rope ladder cannulation. From 2004 on, all incident patients were started on buttonhole cannulation, and prevalent patients were converted to this cannulation method. Coprimary outcomes were arteriovenous fistula-attributable systemic infections and a composite of arteriovenous fistula loss or requirement for surgical intervention. Secondary outcomes were total arteriovenous fistula-related infections and staff time requirements. Additionally, a systematic review evaluating infections by cannulation method was performed.
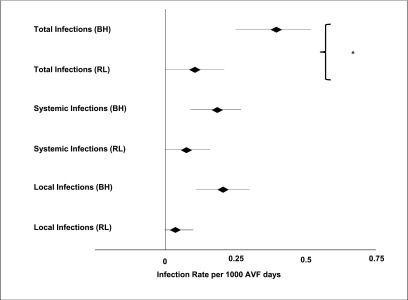
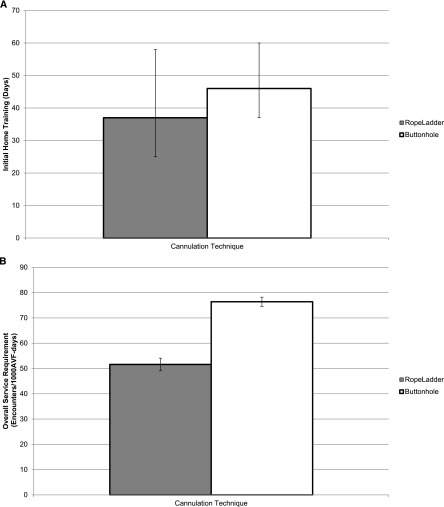
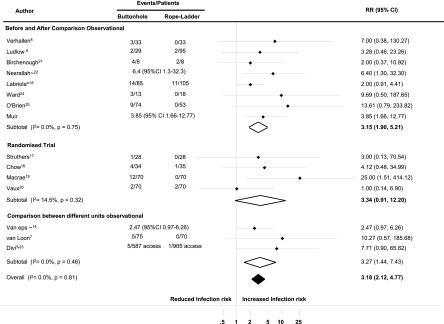
Results: Seventeen systemic arteriovenous fistula-attributable infections were documented in 90 patients who were followed for 3765 arteriovenous fistula-months. Compared with rope ladder, buttonhole was not associated with a significantly higher rate of systemic arteriovenous fistula-attributable infections (incidence rate ratio, 2.71; 95% confidence interval, 0.66 to 11.09; P=0.17). However, use of buttonhole was associated with a significantly higher rate of total arteriovenous fistula infections (incidence rate ratio, 3.85; 95% confidence interval, 1.66 to 12.77; P=0.03). Initial and ongoing staff time requirements were significantly higher with buttonhole cannulation. Arteriovenous fistula loss or requirement for surgical intervention was not different between cannulation methods. A systematic review found increased arteriovenous fistula-related infections with buttonhole compared with rope ladder in four randomized trials (relative risk, 3.34; 95% confidence interval, 0.91 to 12.20), seven observational studies comparing before with after changes (relative risk, 3.15; 95% confidence interval, 1.90 to 5.21), and three observational studies comparing units with different cannulation methods (relative risk, 3.27; 95% confidence interval, 1.44 to 7.43).
Conclusion: Buttonhole cannulation was associated with higher rates of infectious events, increased staff support requirements, and no reduction in surgical arteriovenous fistula interventions compared with rope ladder in home hemodialysis patients. A systematic review of the published literature found that buttonhole is associated with higher risk of arteriovenous fistula-related infections.
Figures
Comment in
-
Should buttonhole cannulation be discontinued?Clin J Am Soc Nephrol. 2014 Jan;9(1):3-5. doi: 10.2215/CJN.11781113. Epub 2013 Dec 26. Clin J Am Soc Nephrol. 2014. PMID: 24370766 Free PMC article. No abstract available.
Similar articles
-
Buttonhole versus rope-ladder cannulation of arteriovenous fistulas for hemodialysis: a systematic review.Am J Kidney Dis. 2014 Dec;64(6):918-36. doi: 10.1053/j.ajkd.2014.06.018. Epub 2014 Aug 8. Am J Kidney Dis. 2014. PMID: 25110302
-
A systematic review of buttonhole cannulation practices and outcomes.Semin Dial. 2013 Jul-Aug;26(4):465-75. doi: 10.1111/sdi.12116. Semin Dial. 2013. PMID: 23859189
-
Home versus in-centre haemodialysis for people with kidney failure.Cochrane Database Syst Rev. 2024 Apr 8;4(4):CD009535. doi: 10.1002/14651858.CD009535.pub3. Cochrane Database Syst Rev. 2024. PMID: 38588450 Free PMC article.
-
Vascular access for intensive maintenance hemodialysis: a systematic review for a Canadian Society of Nephrology clinical practice guideline.Am J Kidney Dis. 2013 Jul;62(1):112-31. doi: 10.1053/j.ajkd.2013.03.028. Am J Kidney Dis. 2013. PMID: 23773840
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
Cited by
-
Guidelines on vascular access for hemodialysis from the Brazilian Society of Angiology and Vascular Surgery.J Vasc Bras. 2023 Oct 30;22:e20230052. doi: 10.1590/1677-5449.202300522. eCollection 2023. J Vasc Bras. 2023. PMID: 38021275 Free PMC article. Review.
-
Buttonhole Cannulation of Arteriovenous Fistulas in the United States.Kidney360. 2020 Mar 6;1(4):306-313. doi: 10.34067/KID.0000052020. eCollection 2020 Apr 30. Kidney360. 2020. PMID: 35372920 Free PMC article. Review.
-
Should buttonhole cannulation be discontinued?Clin J Am Soc Nephrol. 2014 Jan;9(1):3-5. doi: 10.2215/CJN.11781113. Epub 2013 Dec 26. Clin J Am Soc Nephrol. 2014. PMID: 24370766 Free PMC article. No abstract available.
-
Is It Time to Abandon Buttonhole Cannulation of Arteriovenous Fistulas?Kidney Med. 2019 Sep 12;1(5):235-237. doi: 10.1016/j.xkme.2019.07.009. eCollection 2019 Sep-Oct. Kidney Med. 2019. PMID: 32734959 Free PMC article. No abstract available.
-
Should Buttonhole Cannulation of Arteriovenous Fistulas be Used? PRO.Kidney360. 2020 Apr 14;1(5):318-321. doi: 10.34067/KID.0000702020. eCollection 2020 May 28. Kidney360. 2020. PMID: 35369372 Free PMC article. No abstract available.
References
-
- KDOQI: Guidelines for Vascular Access, 2006. Available at: http://www.kidney.org Accessed September 3, 2013
-
- Patel PR, Kallen AJ, Arduino MJ: Epidemiology, surveillance, and prevention of bloodstream infections in hemodialysis patients. Am J Kidney Dis 56: 566–577, 2010 - PubMed
-
- Powe NR, Jaar B, Furth SL, Hermann J, Briggs W: Septicemia in dialysis patients: Incidence, risk factors, and prognosis. Kidney Int 55: 1081–1090, 1999 - PubMed
-
- Taylor G, Gravel D, Johnston L, Embil J, Holton D, Paton S, Canadian Nosocomial Infection Surveillance Program. Canadian Hospital Epidemiology Committee : Incidence of bloodstream infection in multicenter inception cohorts of hemodialysis patients. Am J Infect Control 32: 155–160, 2004 - PubMed
-
- Twardowski Z: The buttonhole method of needle insertion takes center stage in the attempt to revive daily home hemodialysis. Contemp Dial Nephrol 18: 18–19, 1977
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
