

Screening for secondary endocrine hypertension in young patients
- PMID: 24371473
- PMCID: PMC3865118
Screening for secondary endocrine hypertension in young patients
Abstract
Background: Secondary endocrine hypertension accounts for 5-12% of hypertension's causes. In selected patients (type 2 diabetes mellitus, sleep apnea syndrome with resistant hypertension, sudden deterioration in hypertension control), prevalence could be higher.
Objectives: To present etiology of endocrine secondary hypertension in a series of patients younger than 40 years at hypertension's onset.
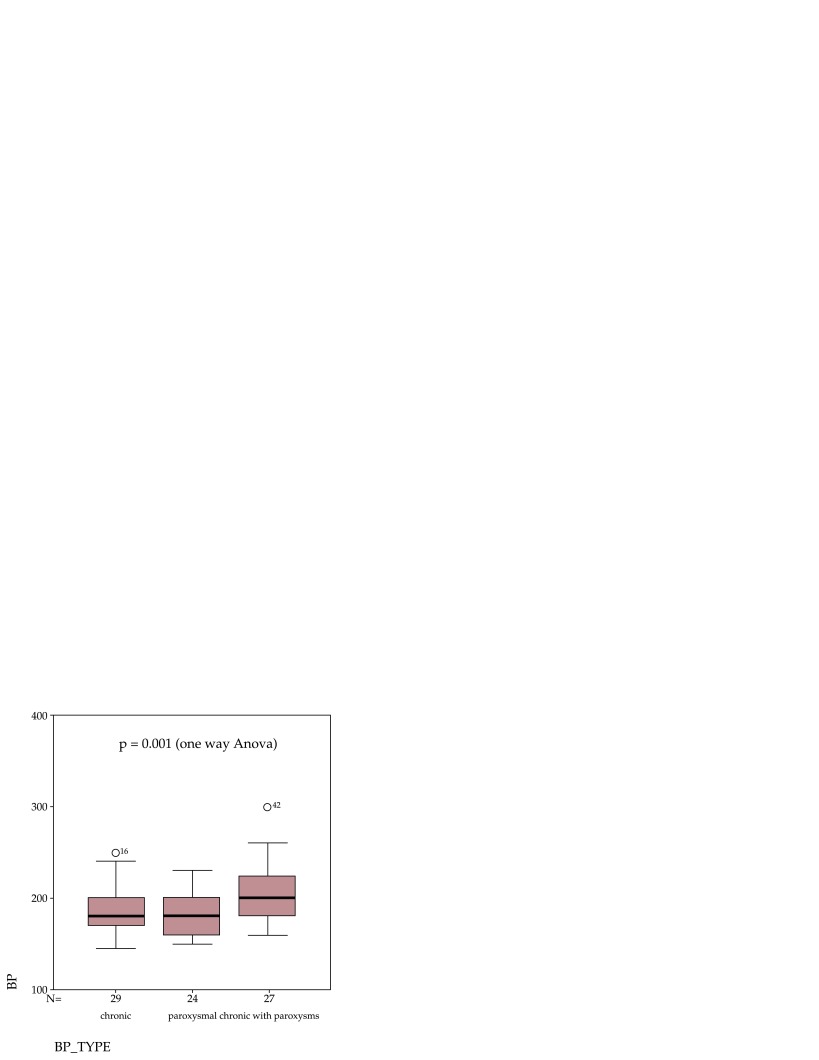
Material and methods: Medical records of 80 patients (39M/41F), aged 30.1 ± 8.2 years (range: 12-40 years), with maximum systolic blood pressure=190.4 ± 29.2 mm Hg, range: 145-300 mm Hg, maximum diastolic blood pressure=107.7 ± 16.9 mm Hg, range: 80-170 mm Hg) referred by cardiologists for endocrine hypertension screening were retrospectively reviewed. Cardiac and renal causes of secondary hypertension were previously excluded. In all patients, plasma catecholamines were measured by ELISA and plasma cortisol by immunochemiluminescence. Orthostatic aldosterone (ELISA) and direct renin (chemiluminescence) were measured in 48 patients.
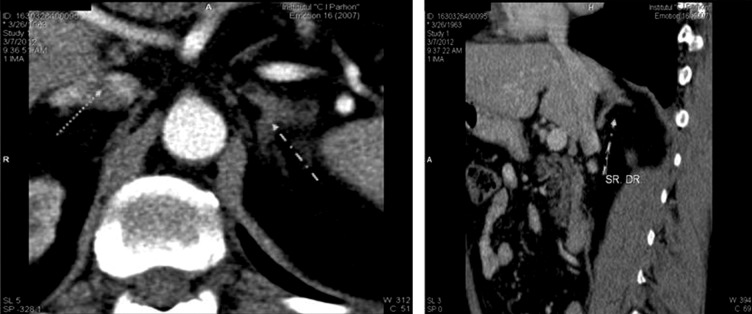
Results: Secondary endocrine hypertension was confirmed in 16 out of 80 patients (20%). Primary hyperaldosteronism was diagnosed in 7 (4M/3F) out of 48 screened patients (14.6%). i.e. 8.75% from whole group: 5 patients with adrenal tumors (3 left/2 right), 2 patients with bilateral adrenal hyperplasia; all patients were hypokalemic at diagnostic (average nadir K+ levels = 2.5 ± 0.5 mmol/L); four patients were hypokalaemic on diuretic therapy (indapamidum); other 3 patients were hypokalaemic in the absence of diuretic therapy. Cushing's syndrome was diagnosed in 6 patients (7.5%): subclinical Cushing due to 4 cm right adrenal tumour - n = 1, overt ACTH-independent Cushing's syndrome due to: macronodular adrenal hyperplasia associated with primary hyperparathyroidism - n = 1; due to adrenal carcinoma - n = 1; due to adrenal adenomas - n = 2; Cushing's disease - n = 1). Pheochromocytomas were diagnosed in 3 patients (3.75%).
Conclusion: Primary hyperaldosteronism was the most frequent cause of secondary endocrine hypertension in our series, followed by Cushing's syndrome and pheochromocytomas. Screening of young hypertensive patients for secondary causes, especially primary hyperaldosteronism, is mandatory.
Keywords: hypercortisolism; pheochromocytoma; primary hyperaldosteronism; screening; secondary hypertension.
Figures
References
-
- Al-Salameh A, Cohen R, Chanson P, et al. Update on Endocrine Hypertension. Article in French. Ann Endocrinol (Paris) 2012;73(Suppl1):S26–S35. - PubMed
-
- Mukherjee JJ, Khoo CM, Thai AC, et al. Type 2 Diabetic Patients with Resistant Hypertension should be Screened For Primary Aldosteronism. Diab Vasc Dis Res. 2010;7:6–13. - PubMed
-
- Di Murro A, Petramala L, Cotesta D, et al. Renin-Angiotensin-Aldosterone System in Patients with Sleep Apnoea: Prevalence of Primary Aldosteronism. J Renin Angiotensin Aldosterone Syst. 2010;11:165–172. - PubMed
LinkOut - more resources
Full Text Sources